HEADER MENU BAR CONTENT INCLUDED IN MASTER PAGEHEADER Menubar
Gastric / Stomach ulcers
GERD - "Heartburn"
GERD - NOT A PROBLEM OF TOO MUCH STOMACH
ACID, BUT RATHER NOT ENOUGH ACID
What is GERD?
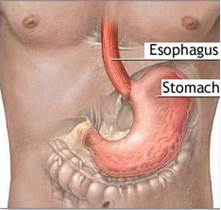
GERD occurs when the stomach's acidic contents flow backward into the esophagus
(sometimes even reaching the mouth).
The esophagus and / or throat is inflamed or damaged by the stomach's highly
acidic hydrochloric acid (HCl) content when the valve between the esophagus and stomach opens at the
wrong time(i.e. other than swallowing) - an inflamed esophagus creates the sensation
of "heart-burn".
GERD can occur in anyone and at any age -but increases substantially for those over the age of 40, with
> 50% of sufferers between 45 and 64;
GERD has become an epidemic problem - especially for those on the standard
Western diet. GERD affects 25-35% of U.S. population
- 10% have it every day, 44% once/month.
The ability of
the esophageal mucosa to withstand injury is a factor in determining whether
reflux disease will develop. Seems to be influenced by age and
nutritional status.
Tissue resistance in the esophagus is determined by the cell
membranes of its epthelial lining and intercellular junctions between them.
These provide protection against
acidic injury by limiting the rate of hydrogen ions (in
stomach acid) diffusing into the epithelium.
The esophagus also produces bicarbonate to buffer
the acid, and mucus, which forms a protective barrier on the epithelial surface.
The resistance of the esophageal mucosa to acid damage is much less than that of
the stomach lining.
When esophageal damage occurs, there is too much acid
and pepsin present for a given level of mucosal protection. The pepsin in the
refluxed stomach acid can damage the esophagus by digesting epithelial protein."
www.gerd.com
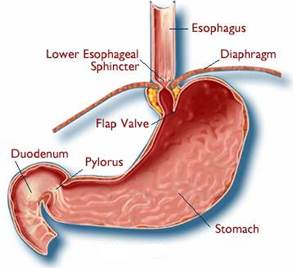
Malfunctioning of GERD-associated sphincters / muscles
GERD involves muscle valves at the top and bottom of esophagus and
stomach, and other muscles. A person can stand upside down after eating a
large meal, and yet no food backs up into the mouth or the esophagus. This is because
muscle rings in the esophagus push food towards the stomach and because of the
mechanical ability of strategically placed sphincter muscle valves. These
sphincters must be working correctly to allow digestive juices to flow correctly
out of the bottom of the stomach - not out of the top.
Meet the "muscle men"
Lower Esophageal Sphincter (LES) (also called cardiac
sphincter, gastroesophageal sphincter or lower esophageal valve). A valve that operates like
a door, letting food into the stomach but preventing it from backing up into the esophagus.
Esophageal Muscles. Ring muscles have peristaltic action to propel food
down the esophagus;
Upper esophageal Sphincter. Closes when you breathe so that air travels
down your "air pipe" and not down your "food pipe";
Diaphragmatic sphincter. Sheet muscle which separates
stomach from upper chest, contains a small opening called the esophageal hiatus,
through which the esophagus passes.
Stomach Muscles. Churn food to aid digestion and move the resulting chyme
through to the small intestine.
Pyloric Sphincter. Located at the pylorus, the outlet at the bottom of
the stomach. This sphincter is stimulated to open and let food out of the
stomach into the small intestine by the parasympathetic nervous system (causes
relaxation).To protect the intestinal lining, the pyloric valve
does not receive the signal to open and release the stomach's acidic contents
into the intestines, until sufficient neutralizing bicarbonate has been released
from the pancreas into the duodenum. Instead, the pyloric valve
constricts more tightly and the LES relaxes, setting the stage for GERD.
Batmangheilidj 1995. Adequate pancreatic bicarbonate production requires sufficient minerals and water:
Abnormal
function of sphincters, esophagus, diaphragm or stomach muscles
Cause
What's Wrong
How Backflow Results
Malfunctioning / Weak LES
MOST GERD HAS THIS PROBLEM
LES is too Relaxed - makes it unable to maintain closure of the gate between stomach and
esophagus.
Impaired /Spastic function does not allow
esophagus to clear or causes LES to open at the wrong time -
possibly due to impaired neuromuscular
mechanisms/neuro-transmitter involvement in resting tone;
Spasticity may be due toMg deficiency /Mg-Ca imbalance.
Leakage - may occur as a
result of damage by H. Pylori bacteria
A weak/malfunctioning LES combined with high
pressure from stomach is able to overcome weak LES "gate"
Hiatal hernia - top part of the stomach
sometimes slides up and bulges through the opening (hiatus) in the
diaphragm
The LES is displaced
above the diaphragm into the chest cavity, causing it to malfunction.
Impaired /spastic muscle function of
diaphragm - could result from impaired neuromuscular
mechanisms / neurotransmitter involvement in resting tone;
Spasticity may be due toMg deficiency /Mg-Ca imbalance.
With the LES above the diaphragm, the LES
pressure is lower resulting in increased risk for backflow. Causes
refluxed material to remain in the esophagus longer (making damage more
likely).
Abnormal emptying or clearance of esophagus
"Lazy" esophagus - Esophageal peristalsis
moves swallowed food/liquids into the stomach. When esophageal muscle
contraction is weak or uncoordinated, moving the food into the stomach
is delayed.
Impaired esophageal muscle function could
result from impaired neuromuscular mechanisms /neuro-transmitter
involvement in resting tone;
Any delay in esophageal clearance or emptying
results in worsening of problems from backflow - By keeping stomach
fluids longer in the esophagus, it increases risk of backflow to throat
and larynx and of irritation and swelling
Gastric Dysmotility - due
toweak (low tone), strong or uncoordinated stomach muscles) -
movement of stomach contents (i.e. chyme) out of the stomach and into
the small intestine is delayed, increasing risk of backflow.
Insufficient stomach acid -
pH >3 triggers stomach lining G-cells to release GASTRIN hormone,
which signals the pyloric sphincter valve to open and let the chyme move
forward and parietal cells to release HCl
Impaired stomach muscles and/or pyloric
sphincter (valve at the bottom of the stomach) - could result from magnesium deficiency or
Mg/Ca imbalance.
Delayed stomach emptying puts back- pressure
on LES due to increased stomach volume.
Some disorders (e.g. diabetes / low blood
sugar; hypothyroidism; paralysis) are associated with delayed
stomach emptying.
Abnormal Function of Upper Esophageal Sphincter (UES)
Possibly due to impaired neuromuscular
mechanisms/neuro-transmitter involvement in resting tone;
Spasticity may be due toMg deficiency /Mg-Ca imbalance.
Stomach fluids in esophagus able to backflow
beyond upper "gate" or UES into throat and voice box
Causes of GERD
the RELATED sphincters / muscles are not
working properly
GERD
happens with relaxation of both the LES and the diaphragmatic sphincter
Could be due to:
Muscle spasms - which in the case of the LES would allow acid to escape
into the esophagus. In particular, an unbalanced intake ratio of
calcium to magnesium(typically a magnesium deficiency, since calcium is
well supplied in Western diet) can cause tight, spastic muscles
throughout the body.
Bacterial infection -such as H. Pylori can damage them;
Neurotransmitter involvement - autonomic nervous system (ANS) uses certain
neurotransmitter chemicals to contract muscles or inhibit contraction
Muscle weakness - is another possibility, but there is really no good
reason for these muscles to suddenly weaken
Certain Medications can Cause GERD
Certain drugs tend to relax the LES valve - causing it to
open during normal stomach gas pressures. The worst (according
to GERD researcher Dr. Mark Hyman):
The channel blockers - used to treat high blood pressure;
Steroids - used for inflammatory conditions: arthritis, lupus;
E.g. Prednisone;
Statins - cholesterol-lowering drugs E.g. Lipitor
Drugs with anticholinergic effects. E,g Tylenol
PM, Benadryl. Inhibit the transmission of parasympathetic nerve impulses that use
acetylcholine to reduce spasms of smooth muscle. E.g. LES, bladder muscles)
Some anti anxiety drugs, bronchodilators,
antidepressants, beta blockers and nitrates(e.g. nitroglycerine);
Some drugs delay the emptying of the stomach -
increasing the stomach's contents, making reflux more likely. E.g. opioids
(opioids also reduce transient LES relaxations (TLESRs)
Compromised bicarbonate buffer and low stomach HCl
GERD Connection to compromised bicarbonate buffering
system. If the bicarbonate buffering system fails, then
there will also be less Hydrochloric Acid produced in the stomach.
Low stomach HCl means digestion is prolonged, which causes gastroparesis,
"delayed emptying" of food from stomach into intestines. An overly full stomach
is more liable to cause reflux.
* Buffers are chemicals that
prevent pH from changing easily by substituting changes in the relative
concentrations of the weak acid and its conjugate base
(formed when the weak acid gives up its proton). Wide fluctuations
in pH (H+
concentration) are prevented by the presence of several weak acid pH
buffers. These weak acids exist in equilibrium with the corresponding
base at physiologic pH. Buffers respond to changes in H+
concentration by shifting the relative concentrations of the buffer and
the corresponding base to dampen the change in pH.
The lower esophageal sphincter (LES) is often involved in GERD
What is the LES?
The LES opens for about 5 seconds when you swallow food and liquid
to allow their passage into the stomach. Otherwise the LES should
stay closed to stop any backflow of stomach acid into the 8-10" long esophagus which would
damage the esophageal mucus lining. Chronic malfunctioning of the LES can lead to
persistent acid reflux, called GERD. Apart from the discomfort, having GERD increases
risk for severe problems such as Barrett's disease and esophageal cancer.
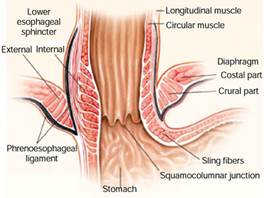
The LES is composed of a smooth musclefibers in the lower 3-4 inches of the
esophagus below the diaphragm in the esophagogastric Junction (EGJ, the junction of the lower end of the
esophagus with the stomach). The LES muscle fibers are in the form of
"C-shaped" fibers (not circular) that "clasp" each other.
and are surrounded by sling fibers over
the upper stomach (fundus). Modulated by neural / hormonal mechanisms, the
clasp-like semi-circular LES muscle fibers have significant myogenic tone,
having
the main control over basal (resting) LES tone.LES contraction is somewhat
controlled by the excitatory motor neurons and LES relaxation is innervated by the inhibitory motor neurons located either locally within
the LES or in the esophagus Brookes SJH et al, 1996.
However, the LES clasp-like
muscles are not as responsive to cholinergic
stimulation (i.e.stimulation by the neurotransmitter acetycholene,
as the gastric oblique sling muscles located over
the stomach. The excitatory (cause contraction) and inhibitory
(inhibit contraction) motor neurons cause these gastric sling fibers to contract vigorously
to cholinergic stimulation (i.e. acetylcholine), dopamine and other agents.
Tian ZQ et al, 2004; Preiksaitis HG et al, 1997
Purpose of the LES
At rest it is contracted - to prevent the contents of the
stomach from flowing backward;
Triggered to relax when there is food in the esophagus -
so that food can pass through to the stomach. After food passes into the
stomach, the sphincter contracts again, closing off the esophagus;
Quickly regains its tone when the food has passed - A
healthy LES opens for only a few seconds in response to swallowing to allow the
passage of food.
The LES Pressure (LESP)
The LES provides a pressure
barrier between the esophagus and stomach. In addition to the LES muscle itself,
the LES pressure is determined by muscles at the bottom of the esophagus as well
as the muscles of the diaphragm that surround the bottom of the esophagus.
When it is closed, the
contraction of the LES maintains a higher pressure than
that of the stomach - so that food and digestive juices cannot
wash back into the esophagus. Mediated by the exicitory vagal motor pathway
(explained below), contractions are consequential to peristalsis-related
relaxation, increased abdominal pressure (to counter back pressure from stomach
fullness), and also, the distal Les contracts in phase with stomach
contractions.
The LES opens or relaxes,
lowering its pressure - as food is moved down the esophagus by esophageal
peristaltic (wavelike) contractions..
How does the lower esophageal sphincter (LES) open and close?
LES CLOSES
The LES contracts (closes as an active process)and thickens when initiated by:
(1) The muscle cells themselves (myogenic). Gastric
sling muscle fibers loop around the esophagogastric Junction (EGJ, the junction
of the lower end of the esophagus with the stomach) and affect LES tone.
Gastric sling fibers
form the oblique muscle layer of the stomach and intermingle with the C-shaped fibers
of the LES. Loss of gastric sling function is thought to be associated with severe
reflux disease.
and
(2) Neural stimulation under autonomic nervous system (ANS,
subconscious / involuntary ) control of the neurotransmitter
acetylcholine via excitatory motor neurons in thevagus
nerve. The LES is classified as an involuntary sphincter (i.e.
nerve stimulation comes from the ANS),
LES opens
The LES relaxes / opens
(a passive process) when you swallow food or drink. The usually,
actively closed LES opens by a
relaxation coinciding with a pharyngeal swallow, when its contraction by excitatory
neurons is inhibited by the innervation of the vagal inhibitory motor neurons
(using neurotransmitters such as Nitric Oxide). (Note that muscle relaxation in vertebrates
is only obtainable by inhibition of muscle contraction - by
inhibiting its excitatory motor neuron. The LES pressure (keeps the LES closed)
returns to its higher resting level after the peristaltic wave to push food
toward the stomach has passed
through the esophagus, such that reflux of gastric juice that may have occurred
through the open valve during a swallow is cleared back into the stomach.
Lump in the Throat ("Globus Sensation"). The classic sensation of a lump in the throat occurs as the upper
esophageal sphincter tightens. It does this to compensate
for a malfunctioning LES which has allowed leakage into the esophagus.
Transient LES Relaxation (TLESR)
Belching and Burping - it is normal for the LES to occasionally open spontaneously
with no swallowing. These TLESRs usually occur after a meal when the stomach is
full and distended, to let air out of the stomach. About 15 mL of air is delivered
to the stomach with each swallow,
and without an in-built venting mechanism, uncontrolled GI bloating
would occur. A backwashing of food and stomach acid into the esophagus can also
occur at this time. Normally TLESRs do not occur while lying flat.
A normal response to a TLESR is to initiate strong esophageal contractions to force
refluxed stomach contents back into the stomach, and so clear the acid from the
esophagus. Saliva neutralizes any remaining gastric acid making it less likely to
injure the esophageal lining. As a result of these mechanisms,
most TLESRs do
not cause heartburn symptoms.
Factors that cause the LES to open
The closing pressure of the LES value at its resting point is about 20 mm of
mercury
Decrease ▼LES Pressure (Open LES)
LES-Relaxing Foods / Drinks:
Tomatoes and tomato-based products like sauces and tomato juice; citrus
fruits and juices; peppermint; alcohol (but also increased stomach acid production);
Highly caffeinated beverages: tea; coffee; colas - caffeine is a
derivative of xanthine . Caffeine effects GABA metabolism levels of the neurotransmitter GABA,
which is made in the GI tract, brain, and the rest of the nervous system. It is important
for managing stress and mood, and will cause the digestive system to remain
calm.
Chocolate - In one experiment, after chocolate ingestion, a mean basal
LES pressure of 14.6±1 mm Hg decreased significantly
to 7.9±1.3 mm Hg; An identical LES response occurred when antacid was given
with the chocolate dose, indicating that gastric alkalization does not affect
the adverse pressure on LES after chocolate consumption. Wright LE
et al, 1975.
Surdea-Blaga et al, 2019
Fatty foods
Mints. peppermint, spearmint
Moderate / Excessive Alcohol Newberry and Lynch, 2019A meta-analysis of 29 studies found that those who had > 5 alcoholic
drinks / week doubled their risk of GERD.
Pan et
al, 2019
PPreserved meats such as cured bacon, hot dogs (contain nitrates, which
are nitric oxide (NO) donors)
Inhibitory Neurotransmitters involved with LES relaxation
/ closing
Nitric oxide (NO)
Vagally mediated inhibition. NO is also involved in smooth muscle esophageal
peristalsis
Vasoactive Intestinal Peptide (VIP)
Activating N-Methyl -D-Aspartate (NMDA) - VIP is an excitatory
neural amino acid released from enteric nerves exclusively in the GI tract
with strong vasodilatory effects on vascular and non-vascular muscle.
VIP can inhibit the contractile activity of gastrin. VIP does not
increase with food intake, but increases in venous outflow of the gut in
response to (1) luminal infusion of fat or acid, (2) electrical
stimulation of extrinsic nerves and (3) mechanical distension of gut mucosa.
VIP secretion is induced by acetylcholine? or neostigmine ( a cholinesterase
inhibitor that is blocked by atropine).
Hormones - cholecystokinin (CCK, stimulates release of bile and
digestive enzymes for protein and fat digestion), estrogen, glucagon,
progesterone (pregnancy hormone), somatostatin, and secretin.
PPeptides - Calcitonin gene-related peptide (CGRP),
gastric inhibitory peptide (GIP), neuropeptide Y, and vasoactive intestinal
polypeptide (VIP)
Conditions:
Reflux is more common when a person is awake and in the
upright position than during sleep in the supine position - When reflux of
gastric juice occurs, normal subjects rapidly clear the acid gastric juice from
the esophagus regardless of their position./li>
Connective tissue diseases (lupus, scleroderma)
Hiatal hernia
Radiation exposure, tumors, infection
Obesity
MMechanical Triggers that initiate innervated inhibition
of the LES - include pharyngeal swallowing and esophageal distention due to food
bolus presence. Note that the esophageal body is not strong enough to force open
the LES if relaxation has not first been mediated by parasympathetic activity
via the vagus nerve;
Some conditions / factors that can cause an increase in your stomach pressure on
the LES
Reduces LES pressure tending to force the LES to OPEN
Gastric or peptic ulcers, gastritis, gastroparesis (delayed stomach
emptying - e.g. occurs with diabetes, when prolonged high blood sugar damages
nerves controlling stomach muscles)
A large meal will displace the liquid contents of your stomach and cause
the liquid level in your stomach to rise.
Late night meals
Fatty foods / especially fried / greasy foods Link - slow down digestion, which increases stomach pressure on LES
and allowing reflux.
Fats take longer to digest than proteins or carbs and so delay gastric
emptying ( (called
gastroparesis)
Effects of fat on gastric emptying,Effects of incorporating
fat into meal on gastric emptying. In some people, high fat foods stimulate release
of bile salts in the stomach, which irritates the esophagus if reflux occurs, and the hormone
cholecystokin (CCK) in the blood, which relaxes the LES - both of which worsen
acid reflux.
Lying down on a Full
Stomach. Your stomach takes an average of three hours
to empty after eating. Lying down too soon puts pressure on LES.
Tight-Fitting Clothing. Wearing tight clothing such as tight
belts/clothes or slenderizing undergarments, squeeze stomach putting
pressure on LES
Overeating / Obesity. Eating large quantities of food or
ill-combined foods or having a large stomach increases stomach gas
pressure.
PPregnancy. the weight of the baby increases
back pressure against the LES in the stomach.
Increase in Transient LES Relaxations (TLESRs)
Those with frequent heartburn symptoms have more frequent TLESRs - compared to
those who have infrequent or no heartburn symptoms. Some people with severe
GERD (and maybe also
Barrett's esophagus), may have a LES with an abnormally low pressure, allowing free
reflux of stomach contents that far exceeds that of the normal TLESRs. In many of
these people, the gastroesophageal flap valve, a fold where the esophagus meets
the stomach, which works in concert with the LES, is open / lax, rather
than closed. Reflux in these people occurs not only after a meal or with burping,
but also at night, and can be brought on by coughing, bending over, lying down,
or wearing a tight-waisted garment. /li>
Neurotransmitters / Hormones / Triggers close the
LES by increasing ▲ LES Pressure
Excitatory neurotransmitters: Acetylcholine, Substance P
Alpha-adrenergic stimulants (promote vasoconstriction) -
norepinephrine, phenylephrine. Studies suggest a significant portion of basal
LES pressure is dependent upon alpha-adrenergic stimulation
Beta-blockers
Muscarinic M2 and M3 receptor agonists - respond to
Acetylcholine
The hormones - motilin (stimulates muscle contractions to move food
through GI tract) and gastrin (stimulates acid secretion in stomach)
The peptides - bombesin (regulates gastric acid secretion by stimulating
gastrin release), B-enkephalin, and substance P (potent stimulator)
Some pharmacologic agents - such as antacids, cholinergics,
domperidone, metoclopramide, and prostaglandin F2α
Treatments for GERD
Standard mainstream treatment for GERD is acid blockers
Acid-blockers are proton pump inhibitors (PPI).
E.g the drug omeprazole. PPI medications reduce acid production, but have side
effects. There is concern that chronic PPI medication can be carcinogenic. Acid-blocking medication is the #3 top-selling drug type
in
America,
and Nexium ("The Purple Pill") and Prevacid are two of the top 10 best-selling
drugs. When acid-blocking drugs first entered the market they were considered so
potent that doctors were warned not to prescribe them for longer than 6 weeks,
and then only to patients with documented ulcers. Prilosec is now available
over-the-counter.
Today, the message is "Eat what you like, then just pop in
a pill".
Serious issues from using acid-blockers
Taking acid-blockers reduces stomach acid (HCl) - they work by neutralizing the stomach acid, so that if it does back-up into
the esophagus, it won’t harm its delicate lining. However,
this cure is worse
than the disease because it reduces your stomach acid, which is needed
to:
Digest protein and food
Activate digestive enzymes
Prevent bacteria (E.g.
H. Pylori) growing in your stomach and small
intestine
Help you absorb important nutrients like calcium, magnesium, and vitamin
B12.
Insufficient stomach acid (HCl) can lead to:
Poor protein digestion - normally
when food is eaten, sufficient HCl is required to produce protease enzymes, such
as pepsin, that break the bonds linking amino acids together.
B12
deficiency leading to depression, anemia, fatigue, nerve damage, and even
dementia, especially in the elderly - For
its absorption, B12 requires a protein made in the stomach, called intrinsic
factor. Intrinsic factor, also required for RBC formation, is not secreted
in adequate levels when stomach acid is low. Ruscin JM et al, Vitamin B (12)
deficiency associated with histamine(2)-receptor antagonists and a proton-pump
inhibitor. Ann. Pharmacother. 2002
Serious
bacterial overgrowth in intestine - called Clostridia, leading to
life-threatening infections;
Stomach
ulcers, GERD and esophageal cancer due to H. Pylori bacteria- these bacteria can grow in the mucous lining of the stomach,
duodenum, esophagus and lower esophageal sphincter (LES) walls when stomach
acidity is decreased to a pH of >= 2.3. It is well established that H.Pylori grows best at neutral pH and fails to survive at a pH below 4.0 or
above 8.2 in the absence of chemicals such as urea. H. Pylori has been strongly linked to ulcers, GERD and esophageal cancer. MD/researcher
Barry Marshall, who researched with Austrian pathologist Robin Warren (Both
awarded the Nobel Prize in Medicine in 2005) demonstrated this when he drank a
Petri dish of H. Pyloriand developed gastritis;
Bloating, gas, abdominal pain, diarrhea, IBS - low-grade bacterial overgrowth in
intestine promotes bloating, gas, abdominal pain, and diarrhea (all commonly
listed acid-blocker drug side-effects). Irritable bowel syndrome (IBS) can
develop as a result of bacterial overgrowth or poor food digestion
Increase in osteoporosis / hip fracture - long-term acid blocking prevents
absorption of calcium and other minerals for bone health. Yang YX et al,
Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA. 2006
Many older people don't have enough HCl in their stomach
- since HCl production declines with age.
Alternative treatments for GERD / "Heartburn"
Dietary changes
Attend to conditions or triggers that cause LES to open
(see above)
Calcium is an essential mineral for muscle tone.
People with GERD tend to have
a weakened lower esophageal sphincter (LES), the muscle that would usually prevent
your stomach's contents from coming back up. It is important to include
sufficient magnesium to
balance calcium presence.
A study of 8 people with heartburn found that taking calcium carbonate caused
an increase in LES muscle tone in 50% of cases. These results suggest that taking
this supplement to improve muscle function may be another way to prevent heartburn
PubMed.
High-fat foods relax the LES muscles, making it easier for your stomach's contents
to reflux back up PubMed. Fats are mainly digested in small intestine. Since fats take longer to digest than proteins and carbs, they delay gastric emptying
-
The stomach emptying its contents at a slower rate is an issue common among
people with heartburn
Effects of fat on gastric emptying,Effects of incorporating
fat into meal on gastric emptying. Delayed gastric emptying has been associated with increased esophageal exposure
to gastric acid and a higher volume of food available to move backward to the esophagus.
These factors would
make heartburn
worse.
Foods / drink that tend to relax the LES muscles, making it easier for your
stomach's contents to reflux back up
The enterochromaffin cells of the GI tract are the most important extra pineal source of
MELATONIN, secreting 400 times more than the pineal gland.
Low
MELATONIN levels are the main cause of insomnia
and lead to GERD by having a negative effect on gastrointestinal motily by its
inhibitory action on gastric acid secretion and its control of the lower
esophageal sphincter (LES) -
melatonin
inhibits
nitric oxide production,.which plays a role in
relaxation of the LES. MELATONIN -
Which is the best choice for gastroesophageal disorders: Melatonin or proton pump inhibitors?
GERD cure using MELATONIN + vitamins + amino
acids
Formula containing melatonin
(6 mg),
l-tryptophan (200 mg),
vitamin B6
(25 mg),
folic acid
(10 mg),
vitamin B12
(50 ug), methionine (100 mg.) and betaine
(100 mg.) was used once a day in a randomized single-blind clinical trial of 351 human
subjects with GERD and compared with the (proton pump inhibitor (PPI) omeprazole (20 mg) and
found to be 100% effective and better than omeprazole alone. Formula was
taken at bedtime.
Continued during the first 40 days of treatment and
Regression of an esophageal ulcer using a dietary supplement
containing MELATONIN
Formula containing melatonin
(2.5 mg),
l-tryptophan (200 mg),
vitamin B6
(200 mg),
folic acid
(10 mg),
vitamin B12
(50 ug), methionine (100 mg.) and betaine
(100 mg) was prescribed for 35 year old patient with chronic GERD to
heal a 6cm ulceration in esophagus.The treatment reduced his pain after
only 2 hoursThe ulcer practically disappeared after 9 months of
treatment
ANOTHER STUDY CoMPARED using
MELATONIN
to PPI in Gerd patients
Kandil et al,
2010 confirmed that melatoninn has a role in the improvement of GERD
in human subjects when used alone or in combination with omeprazole. Meanwhile,
omeprazole alone is better in the treatment of GERD than melatonin alone. They treated
36 human subjects with GERD.
De Souza Pereira R. (2006) Regression of gastroesophageal
reflux disease symptoms using dietary supplementation with melatonin, vitamins and
amino acids: Comparison with omeprazole. J. Pineal Res. 41:195-200.
PubMed
Dial S, Alrasadi K, Manoukian C, Huang A, Menzies D. (2004) Risk
of Clostridium difficile diarrhea among hospital inpatients prescribed proton pump
inhibitors: cohort and case-control studies.CMAJ.171:33-38. [PMC
free article] PubMed
Kalant H. Roschlau (1998) WHE Principles of Medical Pharmacology.
6th edition. New York: Oxford University Press; 1998. p. 558.
Kandil TS, Mousa AA, El-Gendy AA, Abbas AM. The potential
therapeutic effect of melatonin in Gastro-Esophageal Reflux Disease. BMC
Gastroenterol. 2010 Jan 18;10:7.
PubMed
Krausse R, Bielenberg J, Blaschek W, Ullmann U
(2004)In vitro anti-Helicobacter pylori activity of
Extractum liquiritiae, glycyrrhizin and its metabolites. J. Antimicrob.
Chemother.54
(1): 243-246.
Oxford
Journals
Mahady, Gail et al (2005, Nov) In Vitro susceptibility of
Helicobacter pylori to botanical extracts used traditionally
for the treatment of gastrointestinal disorders. Phytotherapy Research Volume 19,
Issue 11, pages 988-991,
Wiley
Newberry C, Lynch K. The role of diet in
the development and management of gastroesophageal reflux disease: why we feel
the burn. J Thorac Dis. 2019 Aug;11(Suppl 12):S1594-S1601.
PubMed
De Souza Pereira R. (2006) Regression of gastroesophageal
reflux disease symptoms using dietary supplementation with melatonin, vitamins and
amino acids: Comparison with omeprazole. J. Pineal Res. 41:195-200.
PubMed
Sivam GP (2001 Mar) Protection against Helicobacter pylori and other
bacterial infections by garlic. J Nutr. 131(3s):1106S-8S.
PubMed
Surdea-Blaga T, Negrutiu DE, Palage M, Dumitrascu DL. Food and Gastroesophageal
Reflux Disease. Curr Med Chem. 2019;26(19):3497-3511.
PubMed
Turco R, Martinelli M, Miele E, Roscetto
E, Del Pezzo M, Greco L, Staiano A. Proton pump inhibitors as a risk factor for
paediatric Clostridium difficile infection. Aliment Pharmacol Ther. 2010;31:754-759. PubMed
Vermeer IT, Engels LG, Pachen DM, Dallinga JW, Kleinjans JC, van
Maanen JM.(2001) Intragastric volatile N-nitrosamines, nitrite, pH, and Helicobacter
pylori during long-term treatment with omeprazole. Gastroenterology.121:517-525.
PubMed
Viste A, Ovrebo K, Maartmann-Moe
H, Waldum H. (2004) Lanzoprazole promotes gastric carcinogenesis in rats
with duodenogastric reflux. Gastric Cancer. 7:31-35. PubMed
Wright LE, Castell DO. The adverse effect of chocolate on
lower esophageal sphincter pressure. Am J Dig Dis. 1975 Aug;20(8):703-7. PubMed
"Ultraprevention: The 6-Week Plan That Will Make You
Healthy for Life", by Dr. Mark Hyman
Gastric dumping syndrome. If you don’t have enough HCl and enzymes to digest
your food thoroughly, you could be subject to the problems of "gastric dumping
syndrome" (or "rapid gastric emptying syndrome" - though it may not be
rapid!), where "food is emptied too quickly from the stomach, filling the small
intestine with undigested food that is not adequately prepared to permit
efficient absorption of nutrients in the small intestine.
DISCLAIMER: The content on this website is intended for
informational, and educational purposes only and not as a substitute
for the medical advice, treatment or diagnosis of a licensed health
professional. The author of this website is a researcher, not a
health professional, and shall in no event be held liable to any
party for any direct, indirect, special, incidental, punitive or
other damages arising from any use of the content of this website.
Any references to health benefits of specifically named products
on this site are this website author's sole opinion and are not
approved or supported by their manufacturers or distributors.