Acid minerals have a
negative electrical charge. (Attracted to the H+ ion).
They include:
chlorine (Cl-), sulfur (S-), phosphorus (P-), and form hydrochloric acid (HCl),
sulfuric acid (H2SO4), and phosphoric acid (H3PO4).
Alkaline minerals
have a positive electrical charge (attracted to the negatively charged
OH- ion). Nutritionally important alkaline minerals include calcium (Ca+),
potassium (K+), magnesium (Mg+), and sodium (Na+). Na and Ca tend to be oversupplied in the typical western diet.
Mild acidosis disturbs Na+/ K+ pump
function / cellular energy production. To compensate for an
overly acidic blood pH, hydrogen (H+) ions are moved into cells, where they
exchange places with potassium ions inside the cells (to maintain electrical
equilibrium inside cell), thus disturbing Na+/
K+ pump function.
Magnesium is anti-inflammatory
Magnesium needed for inflammation-controlling localized "hormones"
Magnesium (also
vitamin B6 and zinc)
are required for the Δ6D enzyme.
This enzyme converts essential fatty acids
in foods into needed active forms, and which eventually convert to inflammation-
controlling prostaglandins and leukotrienes (localized "Hormones", called eicosonoids)
According to the USDA both decreased magnesium intakes
and blood magnesium levels have been associated with an increased CRP in people
of all ages. Numerous studies have
shown that a low magnesium status occurs often in people with diseases that have
a chronic inflammation component, including heart disease, diabetes, high blood
pressure, and osteoporosis."
According to publication by King et al, "Dietary magnesium and C- reactive protein
levels": "Most Americans consume magnesium at levels below the
RDA. Individuals with intakes below the RDA are more likely to have elevated CRP,
which may contribute to cardiovascular disease risk."
King et al,
2005
Another study examined the association between serum
magnesium levels and C- reactive protein (CRP) in
non- diabetic, non- hypertensive obese subjects.
Concluding: "The results of this study
show that low serum magnesium
levels are independently related to elevated CRP concentration, in non- diabetic,
non- hypertensive obese subjects."
Relationship
study
Magnesium intake ↑ Inflammation ↓
Dietary magnesium
connected to lowered diabetes risk. A study by Dr. Ka He of the University of North Carolina
at Chapel Hill and colleagues found a connection between dietary magnesiumand a lowered risk of diabetes/decreasingINSULIN resistance
- also revealed that as magnesium intake
increased, inflammation levels decreased. Dae
Jung Kim, 2011
Conclusion of another study with older, middle- aged
American women: "Our results suggest
that magnesium intake is inversely associated with systemic inflammation and the
prevalence of the metabolic syndrome in middle- aged and older women."
Magnesium
intake
Magnesium prevents calcification of soft tissues
A healthy cell has high
magnesium
and low calcium levels
Up to 30% of cellular energy is used to pump calcium out of the cells.
Inside the cells, normally,
ATP
energy produced by
cell mitochondria is used to power the calcium pumps (Ca2+ATPase)
that transport Ca++ ions across the plasma membrane to maintain an extracellular
calcium concentration ~10,000 times greater than inside cells (Magnesium
concentration inside cells ~10,000 times greater than the calcium concentration)
- impaired cell
membranes or low
ATPproduction (due to lack of
Mg for the
enzymes required for ATP production or any
other reason) means there is insufficient power to pump out the Ca++ ions and
calcium accumulates inside the cell, preventing the cell from maintaining its
normal calcium gradient. In this event, intracellular calcium increases (a
benchmark at the time of death) and there is a relative deficiency of magnesium.If anyone is seriously ill, this deficit must be addressed with magnesium
supplementation, noting that most oral forms are poorly absorbed.
High
calcium / Low magnesium intake contributes to
calcification of tissues
Outside the cells, Mgkeeps calcium
dissolved. Calcium
intake without sufficient magnesium
encourages soft tissue calcification, since the higher the calcium level and the
lower the magnesium level in the extra-cellular fluid, the harder is it
for cells to pump the calcium out.
A relative deficiency of magnesium compared to calcium causes abnormal calcification in soft
body tissues
Extra-skeletal calcification. Beneficial calcification involves calcium and phosphorus and
is a normal process for building healthy bones and teeth. As the ratio of
Mg to
Ca decreases inside cells (which happens as we age and with lower
ATP energy production), calcium that is
supposed to be deposited in your bones and teeth tends to accumulate in soft
tissues (where there should not be calcification), and where it can cause many
health issues, such as strokes, heart attacks and muscle spasms.
Health consequences of calcium accumulation inside cells
(calcification)
Primarily caused by Mg deficiency or Mg/Ca imbalance.
Unable to remove
calcium from cells, abnormal calcium accumulations
(calcifications) build up in soft tissues, and
cell membranes become rigid.This affects cell transport systems, further
decreasing Mg transport and other nutrients, with
significant adverse effects in the body:
Negatively affects detoxification systems, antioxidant systems
and glucose metabolism
Lowers cellular energy production
Nervous system excitation
Muscle rigidity or spasms. As we age, more and more calcium remains
trapped in the muscles and these become more or less permanently contracted,
leading to increasing muscle tension and spasms;
CVD
/ Stroke / Hypertension / Heart attack/Vascular degeneration. As
a consequence of contracting/constricting blood vessels and
hardening/rigidity of the arteries when calcium deposits in artery walls
(arteriosclerosis). This in turn leads to restricted blood flow causing high blood
pressure and inelastic vessels, which may easily rupture causing strokes. Calcium is a component of arterial lesions
and is of course involved in calcification in heart valve. Countries with the highest calcium to magnesium ratios in
soil and water have the highest incidence of cardiovascular disease (Australia
tops the list).
Osteoporosis
Cancer
Wrinkled skin
Calcification of soft tissue
Arthritis - in
the joints and connective tissue
Muscle / Joint inflexibility -contributes to arthritic deformations in later years
Fibromyalgia
Migraine -
excess calcium can stimulate muscular layer cells of temporal arteries over the
temples causing migraine;
Asthma -excess
calcium constricts the smooth muscle surrounding the small airways of the lung,
causing restricted breathing and asthma;
Bone spurs -
from abnormal calcium crystals in bones;
Fusions in skeletal components
(E.g. vertebrae);
Kidney stones
High blood calcium
GI tract disorders
Chronic fatigue syndrome
(CFS);
Dental problems -
cavities
Cataracts
Senility from calcification of
neurons in brain;
Depression and other mood disorders
VLDL triglyceride increase
General mineral imbalances.
incl.
magnesium, zinc, iron and phosphorus;
Interfere with vitamin D activity -which has many health-protecting functions (especially important in cancer
prevention)
Acceleration of aging process
Magnesium has a calming
effect on the nervous system
The neurological effects of magnesium
Mg++(at high extracellular concentration)
reduces electrical excitation by diminishing synaptic transmission.
Achieved via blocking release of acetylcholine into the synaptic gap between neurons.
Mg++ reduces neuronal excitability in its role
as a natural "Calcium Channel Blocker". Mg++ ions (and other ++ cations at mM concentrations)
decrease the activation of certain membrane-bound, voltage-gated
calcium channels, and in limiting the influx of extracellular calcium++ into the
neuronal cytosol, thereby reduce neuronal excitability.
Mg++ reduces pain. By blocking
N-methyl-D-aspartate (NMDA) glutamate receptors, an excitatory neurotransmitter
of the central nervous system; prevents ion-flow at typical neuronal resting potentials.
Mayer, 1987
Mg is a "calcium channel blocker" in neurons
Mg++ at high extracellular
concentrations blocks Ca++influx and diminishes synaptic transmission.
Dodge, 1967
IfMg
levels are low, nerves lose control over muscle activity, respiration and
mental processes. Nerve cells (neurons) need sufficient
magnesium to give or receive messages, without
which they become excitable and highly reactive. This causes the person to become
highly sensitive and highly nervous, possibly resulting in:
Nervous fatigue
Irritability
Restlessness
Disorientation
Tics / Twitches
Hypersensitivity E.g. sharp muscle reaction to an unexpected loud
noise.
Anxiety
Irregular heartbeat
Tremors
Muscle spasms
Confusion
These effects manifest themselves in several well-known
neurological /neuromuscular conditions. Including sleep disorders, the "shakes"in
alcoholics, Parkinson's disease, migraines, pre-eclampsia, suicidal tendencies,
epileptic seizures, pain, SIDS, CFS and psychiatric disorders:
ATP-producing mitochondria are highly concentrated
in cells of the brain and central nervous system. Since neurotransmission
has an avid need for ATPenergy
Magnesium powers
cell "Battery"
First some background on the cell battery and its transmembrane pumps
What is the cell "Battery"?
The Cell "Battery" is the voltage difference across the plasma cell
membrane (a.k.a. the transmembrane potential).
Typically -70 mV in a healthy cell, with outer membrane being more positive than
inside. The charge difference is determined by an imbalance of mineral ions,
such as K+,
Na+, Ca++
and H+, separated on either side of the membrane.
Body'senergy currency
ATPand the protein enzymeATPase.
ATP (adenosine triphosphate) isproduced by ALL of our cells
(by cell mitochondria) to store energy
(as phosphate bonds) to be used for work in the
cell - in an aqueous medium,
energy is
released from
ATP
by the enzyme
ATPase,
which breaks down (hydrolizes) the phosphate bonds in
ATP (into ADP plus a free phosphate ion).
Without the
ATPase
enzyme,ATP's
stored energy can not be extracted.
Some ATPases are transmembrane pumps
that provide an active transport channel for ions, such as
H+, Na+,
K+
, Ca2+ across a cell membrane
- transmembrane ATPases
(pumps) are integral
proteins of the membrane which make it possible for the solute ions /molecules
to diffuse across the membrane against their concentration gradient (i.e. Via active transport) using
energy released by the hydrolysis/ break down of
ATP.
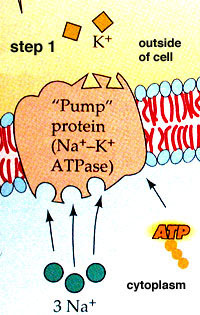
The most significant pumps are:
Sodium/Potassium
pump (Na+/K+-
ATPase) - found
in the plasma membrane of all animal cells; used to maintain the transmembrane
potential (voltage) by powering movement of sodium ions (out of the cell) and
potassium ions (into the cell) across the membrane against
their gradient
Bicarbonate pump (HCO3 -ATP ase)
- present in parietal cell membranes in stomach; used to acidfy the
stomach
Calcium pump (Ca2+-ATP ase) -
Magnesium is necessary to power the transmembrane transport pumps
ATP must be bound to amagnesium ion to be
biologically active. Investigations of the Na/K-ATPase established that
Mg2+ is an essential cofactor for activation
of enzymatic ATP hydrolysis to release
cellular energy
from ATP.
ATP
+ Mg2+ <--> MgATP2-
MgATP2-.
binds to the ATPase enzyme (on the cytoplasmic side of the membrane, without
magnesium being transported
through the cell membrane) and remains bound
throughout the reaction cycle at least until after the release of phosphate.
Most ATPase enzymes break down MgATP2- .
Magnesium also REGULATESATP production -
experimental evidence collected through the years
confirms that Mg2+ ions have a regulatory effect on ion transport by interacting
with the cytoplasmic side of the ion pump. Apell
et al, 2017,
Fukushima & Post,
1978, Mildvan AS, 1987
Effects of having insufficient magnesium available for transmembrane pumps
Lack of magnesium allows cells to swell.
Gradient created by Na/K pump is used
to expel excess water from cell to prevent it from swelling;
Lack of magnesium reduces cell "battery" voltage. The Magnesium-dependentNa/K pumps maintain appropriate
intracellular/extracellular potassium /
sodium
ion concentrations
The Na/K pumps are opened
or closed when stimulated by a change in the cell "battery" voltage - the opening of the
Na/K pump generates an inward
current that affects the membrane potential itself (creating a reinforcing
positive loop).
"No gas (i.e.
magnesium), No Go !"-
a malfunctioning Na/K pump due to a lack of Mg-dependent
ATP reduces the cell "battery" voltage and
mitochondrial ATP energy production in the
cell, which further negatively affects Na/K pumps.
A rat study found that a magnesium
deficiency decreased Na/K
pump activity in heart cell membranes.
Effects of dietary magnesium on sodium-potassium pump action in the heart of
rats.
Chronic magnesium deficiency leads to intracellular calcification
Magnesium is a natural calcium channel blocker, responsible for muscle
relaxation to counter calcium's contraction
Na gradient generated
by Magnesium-dependent Na/K
pumps
is used by cell membrane and endoplasmic reticulum membrane
calcium pumps
(Na+ - Ca2+ translocators,
found in smooth and striated muscle cells) to regulate calcium
concentration in the cell's cytoplasm (i.e.
inside the cell). Calcium
usually enters cells for an excitory action E.g. a muscle contraction or nerve
impulse. Once its job is done, magnesium
empowers calcium
pumps to flush calcium
out of the cell against its gradient, or into intracellular
calcium stores,
such as the sarcoplasmic reticulum of muscle cells or mitochondria of all
cells). A deficiency of magnesium
leads to calcium
accumulation inside cells(called
calcification), which can result in over excitation in nerve and muscle cells. This not
only affects "movement muscle" contractions (seen as spasms), but also affects
heart and arterial contractions.
Familiar health consequences ensue as calcium
accumulates inside cells (calcification).
Including: arteriosclerosis/CVD, cancer,
hypertension, arrhythmias, angina pectoris, neurodegenerative diseases, muscle/joint pain and stiffness,
muscle spasms/ twitching, tension / migraine headaches, painful menstrual
ramping, cataracts, bone
spurs, and on and on . . .
Effects of calcification include:
Inability to relax muscles.
Muscle contraction depends
on a calcium ion concentration bout 10,000 times higher than
its resting concentration
inside cells, which is accomplished by pumping
calcium in via the
membrane calcium
pumps and by using calcium
pumps in the sarcoplasmic reticulum (SR) (a storage depot for calcium, which is a
special type of endoplasmic reticulum found in smooth and striated muscle that
sequesters then releases calcium when the muscle is stimulated to contract).Muscle relaxation occurs when calcium
is quickly returned from whence it came, which may not occur effectively with a
magnesium
deficiency. Magnesium relaxes muscles
Protein/Lipid synthesis
and carbohydrate/steroid metabolism.
In its
role in powering the endoplasmic reticulum membrane calcium pumps, Mg
serves to regulate calcium
concentrations in the cytoplasm by stimulating sequestration of
calcium into the
cell's endoplasmic reticula, which are responsible for:
Synthesis of proteins / triglycerides /
phospholipids / steroids;
Metabolism of carbohydrates / steroids;
Magnesium maintains cell membrane integrity
Magnesium maintains membrane permeability, flexibility and stability by "wearing" several of its different "hats":
Affecting >300 enzymes
Aiding ion transport across cell
membranes
Being involved in fatty
acid and phospholipid metabolism;
Prevents Infection of Cell.
Magnesium deficiency would lead to a weakening of
the cell membrane, thereby setting the stage for infection of the cell. Note
that evidence is building to support the theory that such infections are
involved in cancer.
Membrane integrity affects the ability of cells to prevent calcium from
accumulating inside the cells. A compromised cell membrane (or low
ATP production) makes it difficult for the cell to maintain the normal
concentration gradient of 10,000 times more calcium outside of cells than
inside; when this happens there is increased intracellular calcium.
In vivo,
magnesium deficiency increases
membrane fluidity and permeability.
Heaton et al, 1989
Magnesium needed for cellular and food metabolism
Magnesium is deeply and intrinsically
woven into cellular metabolism:
Mg2+ -dependent enzymes
appear in virtually every metabolic pathway
Specific binding of Mg2+to
biological membranes is frequently observed
Mg2+ is
used as a signaling molecule
Much of nucleic acid biochemistry
requires Mg2+. Including all reactions which require release of energy from
ATP
Magnesiumneeded to metabolize food
Magnesium
is necessary for the metabolism of carbohydrates, fats and amino acids, and many
other biologically active nutrients and substances.
Including calcium, potassium, phosphorus,
zinc, copper,
sodium, lead, cadmium,
hydrochloric acid (HCl), ACETYLCHOLINE, and NITRIC OXIDE (NO).
Magnesium
transports many substances
(E.g. minerals, mineral electrolytes, hormones,
and neurotransmitters)
into and out of cell. Via its
role in maintaining the cell "battery" level
Magnesium detoxifies cells of toxic metals and other toxins
Magnesium protects cells from toxic metals
Magnesium protects cells from aluminum, mercury, lead, cadmium and nickel prevalent in
today's environment. Toxic metal bombardment is a well-known challenge of our modern
day. A consequence of magnesium deficiency
(or relative overabundance of calcium) is lower cell membrane "batteries"(and
thus loss of pumping capacity), such that toxic metals are less effectively
removed from, and thus accumulate in cells. Magnesium
(along with other minerals, such as zinc) is vital for phase I detoxification
and is particularly invaluable for dislodging toxic metals from the body
Evidence is
mounting that low magnesiumlevels allow the
toxic metal deposition in the brain tissue that precedes
Parkinson´s disease, multiple sclerosis
(MS)
and Alzheimer´s
Low total bodymagnesiumcould also be a
major contributor to heavy metal toxicity in children, a factor involved in
learning disorderss
Cellular detoxification
Magnesium
(and other alkaline
minerals)
are utilized by the body for detoxification
Used to process cellular debris
Counteracts elevated uric acid production when combating a
detox reaction. If in short supply,
magnesium is taken from bones
Magnesium is one of the most
commonly deficient nutrients in the chemically toxic individual.
These individuals are observed to excrete high amounts of
magnesium in urine, causing low
magnesium levels in body
The ability to detox a particular toxin varies upon an individual's
magnesium
level. According to Dr. Frederica P. Perera, Professor of Environmental
Health Sciences and Director of the Columbia Center for Children's Environmental
Health, who recognizes that although there can be a 500-fold difference in the
ability of each person to detoxify a particular toxin, a main determining factor
is an individual's magnesium
level
Magnesium
protects the cell from aluminum, mercury, lead, cadmium, beryllium and nickel
Magnesium
has a major role in heart
health / blood pressure
All the usual risk factors for heart disease can be the result of low magnesium
status.
E.g.
hypertension, high total cholesterol, low HDL cholesterol, high LDL cholesterol,
high homocysteine, and high C-reactive protein. Recent
studies show that high anxiety and depression (symptoms of human
magnesium
deficiency) can predict heart disease even more than the traditional risk
factors.
As cofactor in Na/K-ATPase pumps,
magnesium
provides
ATP
energy for heart muscle cells. These have an avid and
constant need for energy.
Mg
levels affect cardiac excitability, contraction, and conduction.
Intra- and
extra-cellular magnesium
levels playan important
role via their regulatory effects on intracellular calcium movement in
heart muscle cells;
Chronic high blood pressure can be caused both directly
and indirectly by a magnesium deficiency
Low cellular magnesium
impedes a healthy sodium to potassium ratio. This is necessary
for normal blood pressure.
Low magnesium :
High calcium in blood vessel muscle cells cause them to contract, resulting in high
blood pressure. Mg levels determine vasoconstriction or
vasodilation via its powerful role in calcium cycling in smooth
muscle of blood vessels:
Highermagnesiumlevels
inside muscle cells produce a relaxing or vasodilating effect
Low
Mg
concentrations inside muscle cells is vasconstricting.
A potential cause of hypertension;
Magnesium
protects the heart from the negative effects of excess calcium.
Mg blocks calcium entry into cardiac (heart) cells and vascular
smooth muscle cells, reducing vascular resistance and naturally lowering blood
pressure.
Magnesium
may act as an anti-arrhythmic agent
Magnesium
limits intracellular calcium overload
triggered during myocardial ischemia This
may be a cause of ventricular arrhythmia; Deranged
intra- and extracellular concentrations of magnesium
, calcium and potassium can manifest as cardiac
arrhythmia
Magnesium deficiency has been implicated and documented in humans.
In atrial fibrillation, supraventricular
tachycardia, torsade de pointes, ventricular ectopy, ventricular tachycardias,
and toxic digitalis arrhythmias.Whang R; Magnesium deficiency -pathogenesis, prevalence, and clinical applications,
Am J Med 82:24, 1987
Magnesium
has an antioxidant role
Magnesium
has an antioxidant role protecting against production of inflammatory cytokines
andROS. Involved with many degenerative diseases
Cardiac muscle necrosis
and lesions were demonstrated in animals fed magnesium-deficient diets.
Necrosis/lesions were consequential to ROS originating from activation of immune
system cells. Weglicki et al, 1996; Weglicki et al, 1992;
Weglicki et al, 1994
Increased susceptibility
to ischemic / reperfusion injury of heart shown in animals fed Mg
-deficient
diets.
Reperfusion injuryis tissuedamage
caused by returning bloodsupply
after a period ofischemia
(restricted blood supply), which results
in inflammation and oxidative damage rather than restoration of normal function.
Weglicki et al, 1994
Magnesium for hormonal balance (crucial to maintaining health)
Magnesium is needed for cholesterol synthesis
(precursor to sex steroids)
Cholesterol
is a prerequisite for all the steroid hormones produced in the adrenal cortex.
Such
as:
ALDOSTERONE. Regulates
body's water and mineral balance, including magnesium
DHEA.
Protects the entire body against the
aging process; prohormone for all the sex steroid
hormones. E.g. Estrogens, PROGESTERONE,TESTOSTERONE;
magnesium deficiency is directly related to
reduced DHEA.
CORTISOL.
Released in response to stress and low blood sugar;
Magnesium status controls uptake and release of many hormones, nutrients and
NEUROTRANSMITTERS
This was concluded by recent research in France and several other European
countries. It accomplishes this via its role in maintaining a healthy cell membrane
potential (Cell "battery" level).
Magnesium
is crucial to the transmission of:
Hormones: E.g. INSULIN, thyroid hormones,
estrogens,TESTOSTERONE,
DHEA;
NEUROTRANSMITTERS: E.g. DOPAMINE, catecholamines,
SEROTONIN,GABA;
Magnesium needed to regulate blood sugar
Intracellular enzyme tyrosine kinase
needsmagnesium to enableINSULINto
regulate blood sugar. And so prevent blood sugar spikes or crashes
Magnesium has a major role in preventing high blood pressure.
Which could otherwise lead to
INSULIN resistance (IR) i.e. INSULIN being
ineffective
Over 300 enzymes need magnesium to function
Mg2+ -dependent
enzymes appear in virtually every metabolic pathway
Magnesium
serves as "gatekeeper" to stop calcium entering into and
activating a nerve - with Mg deficiency, the nerve can become over-activated, which can
cause muscle tension, soreness, spasms, cramps and fatigue, migraine,
and spastic lower esophageal and pyloric sphincter function leading
to GERD;
Keeps heart rhythm steady.
The heart is a muscle - research suggests that cardiac/heart muscle
is more sensitive to magnesium intake than skeletal muscle.
Supports a healthy immune system -
fighting infection
Helps regulate blood
sugar levels. Intracellular enzyme tyrosine
kinase needs Mg to allow insulin
to lower blood sugar
Key involvement in cellular
ATP energy production
Converts
Vitamin D
toCALCITRIOL
(its active form). Crucial in many health functions
Other enzymes that rely on
Mg -
creatine-kinase activation, adenylate-cyclase, and sodium-potassium-ATPase
Helps maintain normal
muscle and nerve function (works together with calcium).
Mg affects cell mechanisms controlling muscle and nerve
cell activity.
Orchestrates the
electric current that sparks through the body's miles of nerves
Promotes proper/strong
formation of bones and teeth
Promotes normal blood pressure. Stimulates production
of prostacyclins and nitric oxide (NO) -both potent artery-relaxing agents.
Promotes normal
bowel function
Involved in protein synthesis
Helps transport
other minerals across cell membranes
Magnesium needed for synthesis of glutathione (the major "in-house" antioxidant)
Glutathione, a primary antioxidant and detoxifier of the cell cytoplasm,
requires Mg
for its synthesis - a major antioxidant produced in
the body, glutathione detoxifies intracellular toxins, such as heavy metals, and
chemicals inhaled from cigarette smoke and car exhausts. Heavy metal presence
increases oxidant damage to cells, which has
long been recognized as a factor in many degenerative diseases.
Glutathione provides a highly reactive
"bulls-eye"for radicals
Glutathione helps red blood cells carry
oxygen
Glutathione is needed for the creation and
maintenance of T-cell lymphocytes -the immune
system's frontline defense against infection
Glutathione is one of the few antioxidant
molecules known to neutralize mercury
According to Dr. Russell Blaylock, low
magnesium is associated with glutathione depletion and dramatic increases in
oxidant
generation. Without the chelating and
antioxidant presence of glutathione, cells weaken under
oxidant damage, setting the stage for
cellular damage and infection, likely factors in cancer, and any of the other
degenerative disease seen today.
For the technobuffs. Glutathione synthetase
requires y-glutamyl cysteine, glycine, ATP, and
magnesium ions to form
glutathione. In magnesium deficiency, the
level of enzyme y-glutamyl transpeptidase is
lowered.
Magnesium is a muscle relaxant
Muscles 101
The function of muscles is to produce force and
cause motion. Either as locomotion of the organism
itself or movement of internal organs.
There are three classifications:
Skeletal muscle. Anchored by tendons to bone to effect skeletal movement, such
as locomotion or posture
Cardiac muscle. Found only in the heart; responsible for pumping blood; similar to
skeletal muscle
Smooth muscle. Found within walls of organs/structures such as esophagus, stomach,
intestines, bronchi, uterus, urethra, bladder, blood vessels; responsible for sustained
contractions.
When referring to the muscular system, "contraction"
means that muscle fibers generate tension with the help of motor neurons.
We use our muscles by selectively contracting them via:
Voluntary (conscious)
contraction of skeletal muscle (controlled by
action potential signals from the central nervous system) .
E.g. movement of quadriceps muscle to kick a ball, or eye
movement occurs as a result of conscious effort originating
in the brain. The brain sends action potential signals
through the nervous system to the motor neuron that innervates several muscle fibers.
In the case of some reflexes, the signal to contract can originate in the spinal
cord through a feedback loop with the brain's grey matter.
Involuntary
(without conscious thought) contraction of cardiac or smooth
muscle (non-conscious brain activity or stimuli from the body to the muscle).
Necessary for survival.
E.g. contraction of the heart muscle for heartbeat,
peristalsis (pushes food through GI tract)
Calcium pumps move calcium powered by
ATP produced by magnesium-dependent
Na/K pumps
Plasma membrane Ca2+-ATPase (PMCA)
pumpmoves calcium into and out of all eukaryote
(nucleus-containing) cells. Ca2+ is an important
second messenger (relays messages from membrane receptors to intracellular
targets), so intracellular levels must be maintained at low concentrations to prevent
noise, in order to have messages delivered properly (called cell signaling).
PMCAand the sodium calcium exchanger (NCX)
are the main regulators of intracellular Ca2+ concentrations.
Since PMCA transports Ca2+ into the extracellular space, it is also
an important regulator of the calcium concentration in the extracellular space.
The PMCA pumps are powered by the hydrolysis of
magnesium-dependentATP (One Ca2+ ion removed for each molecule
of ATP hydrolysed).
PMCA binds tightly to (has high
affinity for) Ca2+ ions but does not remove Ca2+ at a
very fast rate, and is well-suited for maintaining Ca2+ at its normally very low
levels. In contrast, NCX has a low affinity, but a high capacity and is thus better
suited for removing large amounts of Ca2+ quickly, as is needed
in neurons after an action potential.
Sarcoplasmic reticulum Ca2+-ATPase
(SERCA) pump. in muscle cells,
the SERCA pump pumps calcium previously released from cell cytoplasm, back into
the sarcoplasmic reticulum, a cell organelle that acts as a storage depot for calcium
inside the muscle cell.
The
SERCApumps
are powered by the hydrolysis of Mg-dependent
ATP
Magnesium roles in contraction/relaxation of muscle
The Mg-dependent Na/K pumps maintain appropriate
intracellular/extracellular potassium/sodium ion concentrations
The electrical action potential signal in a muscle
cell to initiate a contraction involves complex movement of sodium
and calcium ions into and potassium ions out of the muscle cell to propogate an
action potential and depolarize the cell.
There must then be a rapid restoral of the ions
against their electrochemical gradients for the cell to repolarize and be ready
for the next action potential.
Muscle contraction (The Calcium
Cycle) occurs in response to a nerve's electrical action potential stimulus. Contraction
of cardiac and smooth muscle requires rapid shifting of intracellular calcium
ions to maintain appropriate gradients; a muscle contraction is initiated
when intracellular calcium is released from the sarcoplasmic reticulumor calcium
enters the cell from the outside.
Mg++ levels inside and outside the cell have an important role
in the intracellular calcium cycle in muscle cells
Muscle relaxation requires intracellular calcium to be quickly
pumped back into the sarcoplasmic reticulum - via
magnesium-dependent SERCA pumps and is pumped out of the cell via PMCA
pumps after the calcium cycle is completed.
Mg-dependent Na/K-ATPase pumps
are vital for production of mitochondrial ATP energy needed to enableSERCApumps to quickly shunt Ca++ back into the
sarcoplasmic reticulum and PMCA pumps
to pump Ca++ out of the cell
Magnesium
is a "Calcium Channel Blocker" (for some cell
membrane-bound calcium channels). Magnesium++ serves
as an important gating mechanism limiting the influx of extracellular calcium into
the cytosol via PMCA pumps. Magnesium is thus similar
to calcium channel blocker drugs, which lower blood pressure by blocking calcium
entry into heart and smooth muscle cells of blood vessels.
Magnesium limits the influx of extracellular calcium into the cell
cytoplasm
Magnesium is a muscle relaxant in skeletal muscle contractions
"Do move a muscle"101
The neuromuscular system is the combination of the nervous system and
muscles, working together to permit movement. The brain controls the movements
of skeletal (voluntary) muscles via specialized nerve cells (neurons).
Process to
move a body part. A message (an action potential) is sent to
upper motor neurons, which have long tails (axons) that go into and
through the brain, and into
the spinal cord, where they connect
with lower motor neurons. At the
spinal cord, ~50-200 lower motor neurons in the spinal cord send their axons via
nerves in the arms and legs directly to the muscle they control. Each lower motor neuron is subdivided into many tiny branches. The tip of each
branch is called a presynaptic terminal.
The connection between the tip of the nerve and the muscle is called the
neuromuscular junction.
The neurotransmitter ACETYLCHOLINE
triggers skeletal muscle contraction. The
electrical signal from the brain (action potential) travels down the nerves (neurons) and prompts the release of
the chemical
ACETYLCHOLINE
from the presynaptic terminals. This chemical is
picked up by special sensors (receptors) in the muscle tissue. If enough
receptors are stimulated by
ACETYLCHOLINE your muscles will contract. For skeletal muscles, the force exerted by the
muscle is controlled by varying the frequency at which action potentialsare
sent to muscle fibers.
Magnesium role in muscle tension and spasms
Magnesium
depletion leads to increased neuronal excitability and enhanced neuromuscular
transmission. The
opposite effect occurs with
magnesium excess. An example of acute CNS
magnesium deficiency is
found in cattle with "grass staggers"(tetany), leading to severe muscle seizure
and even death. In humans, a chronic
magnesium deficit is implicated in neurological and neuromuscular conditions,
such as migraine, CFS, and many other sleep and psychiatric disorders.
A
decrease in neuronal magnesium
concentration is postulated to increase calcium binding to prejunctional
ACETYLCHOLINE
vesicles. Increasing release of ACETYLCHOLINE into
the neuromuscular cleft and so increasing muscle contractions.
With a relative deficiency of magnesium to
calcium, calcium remains trapped in the muscle cells.
Over time, if the relative deficiency continues (as often occurs in
aging), the muscles become more or less permanently contracted, leading to
increasing muscle tension and sp
Adequate magnesium is essential for calcium absorption and
metabolism
Calcium (Ca) / Magnesium (Mg) - The classic ying/yang pair
Neither
magnesium or calcium can act without eliciting
a reaction from the other. Biochemically,
magnesium and Ca have complementary and antagonistic roles to each other:
Magnesium has a pivotal role in energy
production and many cellular metabolic processes
Calcium is more concerned with structure strength
(in bones and teeth) and movement
(neuromuscular).
Inside the cell. magnesium is a cofactor with ATP
providing power for the intracellular pumps. E.g. the important Cell "Battery"
Pumps (Na+/K+-ATPase), bicarbonate pumps (HCO3-
ATPase), and calcium pumps (Ca2+-ATPase)
all need Mg2+ATP to maintain effective
ionic gradients within and outside the cell.
Magnesium is the second-most abundant positive
ion (cation) inside the cell, but most is bound to molecules that regulate
energy production, storage and utilization.
Magnesium is required in the mitochondrial respiration cycle (during oxidative phosphorylation
and anaerobic metabolism of glucose);
Magnesium (Mg) /Calcium (Ca) Interplay
Magnesium
keepscalcium dissolved in bloodstream, heart, brain, kidneys/urine, and
in all the tissues in your body. Try crushing a
calcium pill in 1oz water and watch
how slowly adding a crushed magnesium pill enables the
calcium to dissolve.
Prevents kidney stone formation.
Magnesium increases
calcium solubility in urine and Mg supplementation
has demonstrated a significant reduction in recurrence of kidney stones.
An insufficiency
ofmagnesium to keepcalcium dissolved can result in muscle spasms, fibromyalgia, hardening of the arteries
and more.
Magnesium prevents soft
tissue calcification.
The higher the calcium level and the lower the
magnesium level in the extra-cellular
fluid, the harder it is for cells to pump the calcium out.
Insufficient magnesium to ensure smooth running of the
calcium pumps can result in calcification of soft
tissues responsible for a slew of familiar health problems
Activity of many enzymes
depend on a sufficient amount of intracellular magnesium.
Detrimentally affected by even small increases
in levels of intracellular calcium.
Growth of cells, cell division, and parts of metabolism depend
onmagnesiumavailability. This can be compromised if
excess
calcium is present.
Magnesium is essential for
calcium absorption and
metabolism. Conversely, several studies report that increased
calcium intake significantly reduces
magnesium uptake and utilization;
Magnesium maintains proper blood
calcium levels
Magnesium is nature's "Calcium Channel Blocker"
in nerve cells. Calcium enters nerve
cells throughcalcium channels carefully guarded by magnesium, which allows just
enough calcium through to create the necessary electrical transmission along the
nerve cell, and then once the job is completed, immediately helps to eject the
calcium.
Calcium is needed to contract a muscle and
magnesium
is needed to relax it. We use our muscles by selectively contracting
them. Muscle contraction is triggered by calcium ions flowing into muscle cells.
To relax the muscle calcium is pumped out again. Problems, such as muscle spasms,
occur when calcium to magnesium
ratio becomes too high, usually because of a
magnesium deficiency.
Magnesium is needed to maintain the cell "battery"
providing the power for calcium pumps
(Ca2+-ATPases)to pump
calcium out of cells.
Most of the enzymes
(E.g. ATPase) involved in mitochondrial ATP
production require magnesium. Up to 30% of cellular
energy is used to pump
calcium out of the cells;
Magnesium protects against high
calcium intake linked to higher
risk of prostate cancer. A 1998 Harvard School of Public Health study of 47,781 men found those consuming
1,500 - 2000 mg of calcium per day had about double the risk of being diagnosed
with metastatic prostate cancer as those getting 500 mg per
day or less.Those consuming > 2,000 mg had over four times the risk of developing
metastatic prostate cancer as those taking in less than 500 mg.
Commonly today, a high calcium intake is detrimentally out of proportion
with a low magnesium intake
Calcium and magnesium need to be consumed or supplemented
in around a 1:1 or 1:2 ratio. Previously thought needed at
4:1 or 2:1, more recent indications suggest magnesium intake should be at least
on par with calcium to facilitate
assimilation of calcium.
Current research on the Paleolithic or caveman
diets show that the ratio of their diet was 1:1. Eades M, Eades A, The Protein Power Lifeplan, Warner Books,
New York, 1999
Unfortunately, researchers estimate that the
Calcium to Magnesium
intake ratio is approaching an all time high that favors calcium 6:1.
A
result of excessive increases in calcium intake, while
magnesium intake has decreased
or remained unchanged. Calcium is typically coming from a dietary excess of milk
and other dairy products and high calcium supplementation
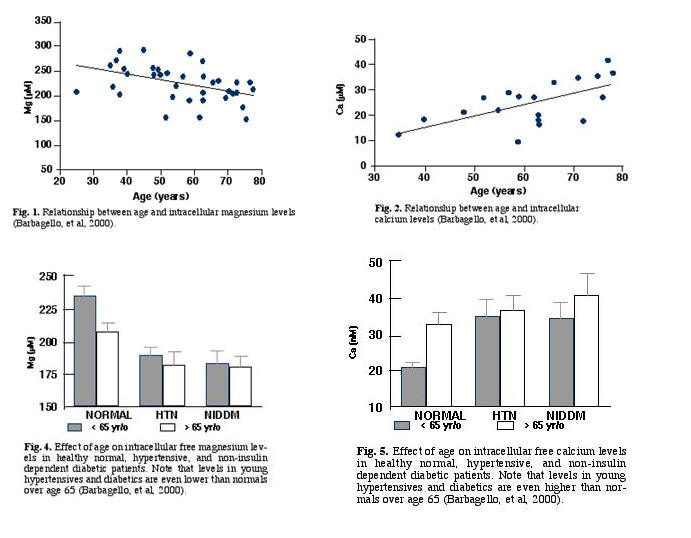
Magnesium (Mg) /Calcium (Ca) ratio changes with age
Intracellular calcium to
magnesium ratio increases with age.
Found a study of 103 subjects of various ages measured intracellular
levels of magnesium and
calcium in red blood cells drawn at 9 AM.
Barbagallo et al, 2000
Highcalcium tomagnesiumratio is clearly involved in hypertension / atherosclerosis
and Non-Insulin dependent Diabetes Mellitus (NIDDM) -
subjects with hypertension or NIDDM had significantly higher levels of intracellular
calcium and lower levels of intracellular magnesium—even worse than the levels seen
in older normal subjects (see Figs. 4 and 5).
Neither age, hypertension or diabetes had any effect
on serum (liquid portion of blood, minus the red and white blood
cells) concentrations of
calcium and magnesium. Only about 1% of magnesium is extracellular, thus serum magnesium
levels do not accurately reflect intracellular magnesium content. Furthermore, only
10-15% of intracellular magnesium is in the free, active form.
Gupta et al,
Younger normal subjects had higher levels of intracellular
magnesium, and lower levels of intracellular calcium (Figs.
1 and 2) than the normal older subjects
Subjects
Healthy
Hypertensive
Non INSULIN dependent diabetes mellitus
<65 yrs
26
30
15
>65 yrs
11
9
12
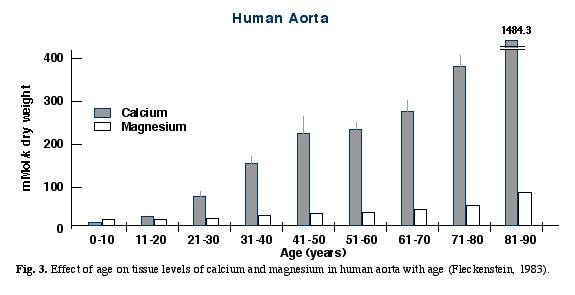
Fleckenstein found similar changes in tissue
calcium
and magnesium levels in the aortas of humans who died at various ages.
Fleckenstein demonstrated the progressive accumulation of
calcium in arterial tissue,
resulting in a shift of the calcium /magnesium ratio in favor of
calcium (Fig. 3).
Fleckenstein A, 1983
Barbagallo, M., Gupta, R.K., Dominguez, L.J., and
Resnick, L.M. (2000) Cellular ionic alterations with age: Relation to hypertension and
diabetes. J American Geriatrics Society. 48: 1111-1116.
PubMed
Dae Jung Kim et al (publ. online Aug 31, 2011 ) Magnesium
Intake in Relation to Systemic Inflammation, Insulin Resistance, and the Incidence
of Diabetes. Diabetes Care,
PubMed
Dodge Jr FA, Rahamimoff R. Co-operative action a
calcium ions in transmitter release at the neuromuscular junction.
J Physiol 1967; 193: 419-432.
PubMed
Fleckenstein, A. Calcium Antagonism in Heart and
Smooth Muscle, John Wiley & Sons, New York, 1983.
Gupta, R.K., Gupta, P., Yushok, W.D., Rose, Z.B.
Measurement of the dissociation constant of magnesium ATP of 31P-NMR and optical
absorbance spectroscopy.
HEATON H.W., TONGYAI S. & RAYSSIGUIER Y. (1989) : Membrane function in magnesium
deficiency. In: (Ref. 2), 27-33.
King DE, Mainous AG 3rd, Geesey ME, Woolson RF (2005 Jun)
Dietary magnesium and C- reactive protein levels. J Am Coll Nutr. 24(3):166- 71.
Pubmed
Mayer ML, Westbrook GL. Permeation and block of N-methyl-D-aspartic
acid receptor channels by divalent cations in mouse cultured central neurones.
J Physiol 1987; 394:
501-527.PubMed
Weglicki WB et al; Role of free radicals and substance P in magnesium
deficiency, Cardiovasc Res 31:677,
1996.
Weglecki WB, Philips TM, Pathobiology of magnesium deficiency -a cytokine
neurogenic inflammation hypothesis, Am J. Physiology, 263:R734, 1992.
Weglicki WB et al, Cytokines, neuropeptides, and reperfusion injury during
magnesium deficiency, Ann NY Acad Sci
723:246, 1994.
DISCLAIMER: The content on this website is intended for
informational, and educational purposes only and not as a substitute
for the medical advice, treatment or diagnosis of a licensed health
professional. The author of this website is a researcher, not a
health professional, and shall in no event be held liable to any
party for any direct, indirect, special, incidental, punitive or
other damages arising from any use of the content of this website.
Any references to health benefits of specifically named products
on this site are this website author's sole opinion and are not
approved or supported by their manufacturers or distributors.