UTI - Learn the basics about The urinary tract and how it gets infected
A UTI occurs when bacteria enter the urinary tract and reproduce
out of control
The main factor determining whether or not
a UTI occurs is the strength of body's defense mechanisms at the time
Overview
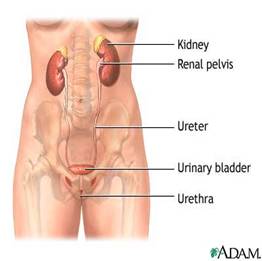
The urinary tract
The male and female urinary tracts are relatively the same.
Except the male urethra is longer
Kidneys. A pair of purplish-brown organs located below the ribs toward the middle
of the back. Kidneys remove excess liquid and wastes from the blood in the form
of urine, keep a stable balance of salts and other substances in the blood, and
produce a hormone that aids the formation of red blood cells
Ureters.
Narrow tubes that carry urine from the kidneys to the bladder
Bladder.
A triangular shaped chamber in the lower abdomen. Urine is stored in the
bladder
Urethra.
Urine in bladder is emptied through the urethra
There are different types of UTIs depending
on location
Urethritis.
An infection limited to the urethra, where most UTIs occur;
Bladder
Infection (Cystitis). UTI spreads from urethra to the bladder;
Kidney Infection
(Pyelonephritis). Untreated, sometimes the infection can
travel up
the ureters to infect the kidneys - a very serious condition.
Bacterial
Prostatitis. Male-only UTI causing inflammation of the prostate
gland;
Instead of a Bacterial Infection,
your problem may be . . .
Candida albicans Overgrowth
Candida
albicans naturally occurs in your body, but gets out of control because of antibiotics,
or antibiotic chemicals (E.g. chlorine in tap water, or sodium fluoride
in toothpaste)
This yeast
can invite the bad bacteria to take up residency by changing the pH of your urinary
tract
Normal urine is sterile and has a slightly acidic pH.
Urine contains fluids,
salts, and waste products and is normally free of bacteria, viruses, and fungi;
Urine's only slightly acidic pH allows it to control growth of many microorganisms.
The bacteria that cause most UTIs like a more acid environment,
but produce alkaline waste that will eventually slow down their own growth;
Healthy pH urine levels are 6.0 - 6.5
in the morning and 6.5 - 7.0 in the evening.
The higher morning acidity
is due to decreased pulmonary ventilation that causes respiratory acidosis during
sleep.
Urine pH can vary from 4.4 - 8. When the body ingests
too many acid-forming foods/drinks, the acid can be buffered using alkalizing minerals,
such as calcium, potassium, magnesium, sodium (borrowed from bone if not in diet).
Excess acids can also be excreted via urine, however, a urine pH below 6.0 (morning)
or 6.5 (evening) suggests that the body's buffering system is overwhelmed.
Diet rich in citrus fruits, most vegetables, and legumes will alkalize the urine.
A diet high in meat and cranberry juice will make the urine
more acidic.
Microbial resistant properties of bladder
lining, and prostate fluid (in men);
Flora maintain bacterial balance in anterior
urethra (part of urethra closest to where urine comes out of
body). Commonly colonized with normal flora, which usually maintains
a balance with bacterial contaminants, e.g. from rectum, skin, or vulva.
Frequent urges to
urinate. Frequent feeling that you have to go very badly and right away
(especially at night, called nocturia), and then there is not much urine to void
Lack of
control over passing urine. Sometimes incontinence.
Painful, burning sensation when urinating (Dysuria). Pain goes away during
urination and immediately returns. Also,
increased difficulty in starting the urine stream
Cloudy urine with foul odor.
Sometimes with
blood in urine
Flu-like, systemic low
fever and aching
A feeling of heaviness
or pain in the lower abdomen over bladder or pubic area
Abdominal pain / Tenderness in the rib area.
Radiating to back on affected
side
Painful voiding of urine (dysuria)
Kidney / Lower back pain.
On side involved, also bladder
tenderness
Fever, headache, nausea and vomiting.
Sometimes delirium, tiredness
UTI Causes / Risk
factors
A UTI is usually caused by an over-proliferation of certain
pathogenic / virilent strains of bacteria taking up residence in urinary tract
wall
These
bacteria should not be in the urinary tract in large numbers.
These misplaced bacteria damage and inflame the mucus membranes and
walls of the urinary tract, resulting
in typical UTI symptoms.
Pathogenic
bacteria typically enter the bladder via the urethra. However,
infection may also occur via the blood or lymph.
it is well established that
colonization of the vaginal mucosa with bacteria from the GI tract precedes the
presence of bacteria in womens' urine.
Most recurrent UTIs are caused by
reintroduction of bacteria from faeces. Schaeffer, 1979
A UTI occurs when E. Coli
"families" take up residence in the
urinary tract wall
~80-90% of UTIs are caused by the bacterium
E. Coli
E. Coli
normally lives in the colon, where it enjoys a symbiotic relationship with us, helping
to break down our waste. E. Coli does not belong in the urinary tract.
To colonize and cause
an infection, E. Coli have little "velcro-like" projections
that adhere to the bladder
(or other UT) wall
linings to prevent their removal. Hair-like projections
(called pili) on the cell surface of E. Coli bacteria contain glue-like
lectin glycoprotein molecules, that adhere to uroepithelial cells lining the
bladder or urinary tract walls to form multicellular communities, called a biofilm. Once the
E. Coli is adhered, it is protected from
being flushed out by urine. How they adhere is not definitely known, but Ofek et
al suggests thats sugar residues on the surface of uroepithelial cells may serve as
receptors for the binding of some E. coli strains
Ofek, 1978.
In vitro tests using uroepithelial cells
from premenopausal women with no UTI history showed that adherence is
maximal at pH 4 to 5 and at
bacterial-to-epithelial-cell ratios of 5,000 or more, suggesting that there are
a limited number of receptors on the epithelial cell surface; adherence tended
to be higher during the early (estrogen-dependent) phase of the menstrual cycle
and diminished shortly after the time of expected ovulation; the
same E. coli strain which adhered avidly to uroepithelial cells from some
individuals barely adhered to cells from other women; Schaeffer, 1979
Getting to know E. Coli
This E. Coli
is not the same as its mutant species associated with unsanitary food processing.
The mutant species has hospitalized and killed people.
E. Coli
thrives in an acid environment
E. Coli
even thrives in acidic urine conditions with a pH as low as 2.
It is capable of synthesizing its nutritional requirements from
the surrounding acids in its environment
After arrival,
the typical E. Coli activity cycle in your urine is that you increase urine
acidity:
By becoming dehydrated
or by drinking/eating acid-containing or acid-forming foods
or drinks that have a predominantly acid effect (E.g, cranberry juice, soda,
lots of sugar)
E. Coli (and other
gram-negative bacteria)
have a burst of growth until they use up all the acid.
At that point their alkaline waste and
endotoxins, which they are living
in, drastically slows their multiplication rates and they become semi-dormant
Less acidity
after menopause reduces infection risk. Lactobacilli
(beneficial organisms) increase the acidic environment in the female urinary tract.
Reductions in their number (E.g. occurs with estrogen loss after menopause) increase
pH and therefore the risk of infection
E. Coli
is a hardy critter and is hard to kill. Here are
some of its virulence factors:
Multiplies fast.
Can double its colony in 20 minutes
Not fussy about
where it lives. Thrives on medical equipment, catheters,
hands, mouth, nose, any mucous membrane, in hair, bladder, on a towel, door handles,
toilet seats, in tap water
Needs just a little
moisture. Air provides enough
Feeds on
almost anything. Can synthesize its own amino acids, purines
and pyrimidines using the nitrogen donor molecule, glutamine (Berks,2002
Can grow aerobically
and anaerobically
Lives in human temperatures (a mesophile). Optimum growth occurs at 25 - 40 °C, but can also survive freezing and boiling temperature
Abigail F. Weliver, Heat as a Microbial Agent
Can quickly mutate
to resist antibiotics. Can actually live on soap!
Can produce a
capsule (outer protective layer) to resist phagocytosis
(engulfment) by immune system
Produces Type
II toxins that damage host cell membranes
Produces cell
wall components that trigger damaging inflammatory response -
E.g. Lipopolysaccharides (LPS), also called endotoxins
The other 10-20% of UTIs are mainly caused by:
Staphylococcus. S. saprophyticus
accounts for ~5-10% of UTIs, mostly in younger women;
Klebsiella(gram-negative, another
acid-lover),
Enterococci
Proteus mirabilis (grows more slowly than
E. Coli
in acid pH; produces uric acid (urea) as waste product; this bacteria WOULD be slowed
down by increasing urine acidity with such as cranberry juice). Generally, cause UTI's in older women;
MORE
RARELY.
Chlamydia trachomatis (intracellular
bacteria i.e.only reproduces inside human cells),
Mycoplasma hominis
(bacteria lacks cell wall, therefore unaffected by common antibiotics)
Since Chlamydia and Mycoplasmamay
be sexually transmitted, infections require treatment of both partners.
These bacteria cannot be treated with d-mannose.
Neisseria gonorrheae {may cause
UTIs in both men and women, but these infections tend to remain limited to the urethra
and reproductive system).
Over-acidity of urine increases risk of UTI
Mildly acidic urine curbs
bacterial growth better than stronger acidic urine. Researchers at
the Washington school of medicine found that urine with an acidic pH close to
neutral was better able to restrict bacterial growth than more acidic
samples. The less acidic samples also had a higher activity of an immune system
protein (siderocalin) that the body makes to fight infection.
Shields-Cutler, 2015
Urine becomes more acidic with:
Dehydration
Dietary "triggers"
causing acidity in the system. Body tries to "dump"
acid via urination;
Being a woman increases risk of UTI
Females are at greater risk for UTIs due to their anatomy.
Men are not as prone as
women to having UTIs. In 95%
of cases, the bacteria enters the urinary tract by the ascending route through the
urethra. Possibly coming from fecal material, use
of spermacides, or the use of diaphragms. The longer
male urethra offers an explanation for why more women than men contract UTIs.
Also, in men, the prostate gland produces secretions that slow
bacterial growth.
Frequent Douching.
Normally, cells in the bladder are coated with a mucus called
glycosaminoglycans(GAGs) -which prevent bacteria from sticking to the cells
in the bladder wall so the bacteria cannot "Set up house".
If that layer of mucus is removed by frequent douching), the bacteria can move in
and grow rapidly.
Wiping forward / Incomplete wiping after a bowel movement contaminates
skin
Use of: diaphragms / spermicides / tampons, sanitary
pads, fragranced feminine hygiene sprays, chemical douches, diaphragm, soap,
bubble baths, toilet paper. Allows chemicals to enter
vagina / urinary tract.
Pregnancy, menopause
Heavy painful menstrual periods
injury to urinary tract. Possibly intercourse
or childbirth increases irritation to give bacteria a new place to grow
Frequent or "first-time" intercourse.
Note that UTIs are not usually a sexually transmitted
disease, but the physical act of intercourse can cause local irritation in the ureter
due to prolonged, frequent, recent or first-time sexual activity, increasing susceptibility
risk to UTI bacteria.E.g. "Honeymoon cystitis" is not uncommon in women
having sex for the first time.
Menopause. Decrease in
estrogen thins the
lining of the urinary tract, which increases susceptibility to bacterial infections.
Other factors increase risk of UTI
Poor hygiene
Overuse of
antibiotics
Impaired
immune function
Not emptying bladder. The
bladder immediately tries to empty itself when bacteria enter. If you are unable
to completely empty your bladder, you have a greater risk of getting an infection -
also, the infection is more difficult to treat
Catheter or tubes placed in bladder
Allergies / Decreased immune function
Lowered libido
Pelvic congestion from chronic constipation
Those with untreated diabetes, spinal
cord injury, M.S., prostate infection
(1) Kill UTI-causing bacteria using a mainstream or alternative antibiotic
First note: you will need to take probiotics after
using any antibiotics
After using antibiotics
(especially prescription ABs) you will need to repopulate the healthy, infection-fighting
bacteria in your gut by taking probiotics or you will "Win the Battle, but
Lose the War". Taking prescription,
or even some natural / alternative, antibiotics will kill a bladder infection, but will also kill the
body's healthy
bacteria (i.e. normal flora that prevent pathogenic bacteria from growing), setting you up for yeast overgrowth,
development of antibiotic-resistant strains of infecting bacteria, and
other problems, cumulatively compromising your long-term health.
After infection is gone, take a good
probiotic supplement (containing at least 50 BILLION CFU of several different
bacteria / daily dose) for at least a month or two.
This should restore natural flora destroyed by antibiotics. However, if you did
not prolong your use of antibiotics, you may regain balance to flora by simply using "kitchen"
probiotics, such as yogurt and fermented foods
For example, the
good bacteria known as Lactobacillus plantarum (in fermented foods,
such as pickles, sauerkraut, kimchi, sourdough), naturally
protects the urinary tract (does not include vagina or anterior urethra).
L. plantarum produces hydrogen peroxide,
which destroys bacteria that cause infection;
Some prescription
antibiotics have been reported to breed super-resistant strains and more saliently,
DESTROY the body's microflora. These exist as the first line of defense against such infections. Unfortunately,
we face a huge exposure to antibiotic residues through meat and poultry consumption.
In 2017, over 24 million pounds of antibiotics were sold for use in
food-producing animals in the U.S. to promote economically efficient
growth (about half of the antibiotics sold for use in livestock are also used in
human medicine).
Grapefruit Seed
Extract. As soon as you feel the symptoms coming on, take 250mg GSE (tablet or liquid
form) 3 times daily. ( 250mg GSE is equivalent to 7 drops of maximum strength GSE
Citricidal® liquid). GSE kills UTI-causing bacteria by preventing them
from breathing. Ionescu, 1990
Juniper extract. Bactericidal agent that is safe, won't kill the good bacteria, and has
been shown effective against antibiotic resistant strains of bacteria that cause
UTIs.
Flush out bacteria by
drinking plenty of FLUID every day. Preferably water or unsweetened juices; the ureters
and bladder normally prevent urine from backing up toward the kidneys, and the flow
of urine from the bladder helps wash bacteria out of the body.
When you urinate, force it out with as much pressure as you can apply. This enables water to work by literally flushing your "pipes".
D-mannose detaches E. Coli from urinary
tract (UT) wall to be flushed out in urine
What is D-mannose and what does it do?
D-mannose is a simple, white, crystallized sugar, similar to glucose, that occurs in some plants.
E.g. cranberries, red currants, gooseberries, other berries, peaches, apples,
tomatoes and some vegetables. The D-mannose
supplement is derived from the bark of certain trees. Absorbed from the upper
intestine 8 times slower than glucose, it has a much lower glycemic index than
glucose and does not cause yeast over-growth.
D-Mannose can be used to remove the E. Coli
bacteria causing a UTI from the bladder (or other area of the UT).
Unless your urine is tested, you don't usually know which type of bacteria is
causing the UTI, however, it is estimated that E. Coli is the culprit in 80-90%
of UTI cases, so it may be worth just trying it. D-mannose will not work for NON E. Coli
infections, so if D-mannose doesn't show
significant improvement after about 24 hours, the infection is probably not E. Coli.
E.g. Infections caused by Chlamydia, Mycoplasma and N. gonorrhea DO
NOT respond to D-mannose treatment, and will need an anti-bacterial treatment.
D-mannose doesn't KILL good or bad bacteria, it
just removes them from urinary tract.
Compare with mainstream antibiotic treatment which radically changes GI
bacterial populations required for good health, D-Mannose removes "bad"
bacteria by detaching them from the UT wall and then voiding them in urine.
A kind of prebiotic, D-mannose fosters the growth of good bacteria in the GI
tract.
D-mannose has no caloric effect and doesn't interfere
with blood-sugar regulation even in diabetics. This is because the body metabolizes only small amounts
of D-mannose and excretes the rest in the urine. D-mannose is not stored in the
liver, and being absorbed from the GI much slower than glucose, has a low
gycemic index.
D-mannose at work. Fortunately, E. Coli's hair-like projections
(pili) that stick to the bladder /UT wall stick to
d-mannose even better. When a sufficient dose of D-mannose is
taken, it spills into the urine, literally "sugar-coating" all the
E. Coli's "sticky fingers", including the free-floating E. Coli
and those already "stuck" to the UT walls. The E. Coli complex
formed is then washed away with the next urination. For more information about
how E. Coli operates:
In all but 2 of 43 women (av. 47 yrs of
age) with an active UTI (acute uncomplicated cystitis) had
improved symptoms after taking d-mannose. They took 1.5 grams d-mannose
twice daily for 3 days and then once a day for 10 days. After 15 days, cultures
were negative for UTI infection in 39 (90.7%) of patients. Pretty impressive! Symptoms
showing significant improvement were dysuria (painful urination), frequent voiding,
urgency, tenesmus (coninual/recurrent inclination to evacuate the bowel) and suprapubic
pain.
Prophylatic d-Mannose
prevented recurrence. One month later the 43 patients were consecutively
randomized into two groups: Group 1 (n=22) received prophylaxis of D-mannose one
week / month every other month. Group 2 (n = 21) were untreated. of those
receiving prophylaxis, only 1 woman (4.5%) had a recurrence within 6 months, whereas
recurrences occurred in 7 women (33.3%) in the untreated group. Rate of recurrence
in other studies is typically 15 - 53% in a 6 or 12 months period. DOMENICI,
2016
Daily dose of 2 g d-mannose was superior to placebo
in preventing UTI Wellens et al, 2008
D-Mannose shown to inhibit the adherence of intact bacteria
to epithelial cells. Ofek, 1977
in vitro tests showed that for several E. Coli
strains, D-mannose inhibited adherence to uroepithelial cells by 76 to 100%;Ofek,
1978
D-mannose powder was associated with a signficant recurrence
reduction of bladder infection in women. D-mannose powder was given
to 308 women with a history of recurrent bladder infections after the completion
of antibiotic treatment. Participants were randomized to D-mannose powder (2 grams
in 200 milliliters of water per day) vs a daily oral antibiotic vs no prophylaxis.
After 6 months, D-mannose was associated with a significant reduction in recurrent
bladder infections when compared to both antibiotic and control groups. Women experienced
fewer side effects (nausea, skin rash, headache, vaginal burning) with D-mannose
compared to the antibiotic. Kranjcec,
2014
D-Mannose dose
Powder is the most economical form.
The slightly sweet powder is practically flavorless,
but actually tastes good when dissolved in a glass of water or juice. D-mannose
is also available as capsules (avoids fillers sometimes added to powders), but you
may have to take up to 4 -500mg capsules to obtain required dose.
For treatment of an active UTI: 1.5 grams
twice/day for 3 days, and then 1.5 grams once/day daily for 10 days (Alternatively - take 1 gram three times /day for 14 days)
To prevent the return of frequent/chronic UTIs: 2
grams once/day or 1 gram twice/day
Expect the infection to be considerably better within
24 hours, if not, it is probably not being caused by E. Coli.
If D-mannose is taking care of the problem, ensure you flush out all E. Coli bacteria
by continuing taking it for a few days after symptoms subside, maybe at a slightly
reduced dose or less frequently
D-mannose in food will not clear a UTI. Mannose
is one of the easier essential sugars to obtain from our diets, but it does NOT
occur in sufficient amounts required to stop a UTI.
Where to obtain D-mannose? Supplemental d-mannose powder is readily available for
purchase. E.g. ClearTract Powder, NOW Foods D-Mannose powder
(85g cost < $20).
(3) Alkalize urine / bladder
Alkalizing the urine helps neutralize a UTI by
reducing acidity (raising the pH / alkalinity)
closer to a neutral pH level (overly acid conditions
are often present with a UTI).
Baking soda
Take 1
tsp. baking soda (sodium bicarbonate) in 1 Cup
water 3 times per day until symptoms resolve.
The taste of this drink can be improved by adding the
juice of 1/2 a lemon or lime and using soda water instead of plain water. If using
liquid GSE, the drops can be added to this drink.
Calcium citrate tablets
When
symptoms are strong, take 2000 mg calcium citrate
(2 - 1000mg tablets) per dose with 8oz water at mealtimes ,
three times per day until symptoms decrease,
then take 2000 mg per day, until UTI is gone.
Take
at least 3 hours before bedtime.
Since it may cause irritation as
it sits in the bladder overnight;
Other alkalizing tactics
Potassium citrate, magnesium citrate, or sodium citrate will also alkalize
the urine
Lemon / Barley
water. Helps control infection ; Boil
barley until tender, then drain and drink water with added fresh lemon juice
A diet
high in citrus fruit or vegetables can increase urine pH
(make more alkaline);
It is
probably NOT a good idea to drink cranberry juice.
If the offending bacteria is E. Coli (90% of cases),
it will increase urine acidity, providing a "Happy Hotel" for E.
Coli visitors.
(4) Optional vaginal douches
The following therapeutic douches can correct bacterial
imbalance in the vagina and anterior (lower)
urethra
Plain Yogurt Douche. Yogurt
must be plain and contain active lactobacillus cultures; may be diluted with water.
Another idea is to freeze some yogurt in an empty tampon tube for insertion into
vagina, or simply soak a tampon in yogurt for insertion. Instead of yogurt you can
mix some probiotic lactobacillus powder with water to make a thin paste to use as
a douche
Optional herbal cleanse for kidneys, bladder
& rest of
urinary tract. Dr. Schulze kidney/bladder tea and
formula is a good choice. Cleanses the urinary tract, maintains healthy bladder and
kidneys and dissolves deposits in the kidneys.
Destroys beneficial vaginal flora. A healthy
vagina contains beneficial bacteria and other organisms called the vaginal flora.
The normal acidity of the vagina controls the number and type of bacteria. Douching
can change this delicate balance, making a woman more prone to vaginal infections;
Douching can also spread existing vaginal infections.
Up into the uterus, fallopian tubes, and ovaries;
Chemicals in fragranced douches irritate vaginal lining and increase susceptibility
to infection
Preventative measures against UTIs or their recurrence
Water
"The Solution to Pollution
is Dilution"
Drink more water and less alcohol.
Drink 8 glasses of water/day to keep urine from becoming too acidic; minimize alcohol
intake (alcohol is a diuretic);
Eliminate / Minimize bladder irritants
Dietary Sugar / refined starches (E.g. white flour)
Nicotine, caffeine,alcohol(a diuretic);
Herbal support for bladder, kidneys, urinary tract
Dr. Schulze kidney/bladder tea and
formula. Cleanses the urinary tract, maintains healthy bladder and
kidneys and dissolves deposits in the kidneys.
Consume / Supplement alkalizing minerals -
especially magnesium, calcium and
potassium
Apple Cider Vinegar (ACV) as UTI preventative.
ACV for a UTI is controversial. The reason is that a couple
hours after ACV is FIRST taken, it causes the urine pH to be more acid for a couple
of urinations. However, the next day and thereafter the alkaline minerals provided
by ACV make urine more alkaline. Drink 1 teaspoon - 1 tablespoon RAW Apple
Cider Vinegar in a glass of water or juice 2-3 times a day.
Probiotic Supplementation.
Taking a good probiotic (containing at least 50 billion CFU of several
different bacteria/ dose) has been shown to curb UTIs by providing natural flora
as the first line of defense against "invaders"in the UT, vagina and
anterior urethra (area closest to where urine comes out);
Yogurt. Make plain
yogurt containing active culture a regular part of your diet to improve natural
flora. Lactobacillus plantarum (in fermented foods, such as pickles, sauerkraut, kimchi, sourdough)
- protects the UT (not vagina and anterior urethra) by producing hydrogen
peroxide against "invader" microbes.
Vitamin C
Vitamin C.
Another controversy exists over whether
ascorbic acid increases urine acidity; An old study with guinea pigs (like humans,
they also can not produce their own
Vitamin C) showed that
moderate doses of ascorbic
acid in natural form (E.g. in fruit or orange juice) is well-retained by
the body and does not show up in the urine; interestingly taking an
ascorbic acid supplement
together with baking soda enhances the body's retention of
ascorbic acid, compared
to taking ascorbic acid
alone;
Add 1/8 - ¼ tsp. (~500-1000mg) powdered Vitamin C and 1/3 tsp. baking soda to cool
drinks 3 times /day. This should render a slightly alkaline/neutral
urine pH; alternatively, take an alkaline form of
Vitamin C, such as magnesium citrate;
Drink moderate amounts of juice containing natural Vitamin C .
However, too much will make urine acidic
D-mannose
To prevent the return of frequent / chronic UTIs: Take 2
grams D-mannose once / day or 1 gram twice / day.
Results using cranberry juice / extract for a UTI have been mixed
100% cranberry juice / Concentrated cranberry extract
supplements help PREVENT an infection but do NOT TREAT it (cause urine to become too acidic (favorable to bacterial growth) DURING
a UTI). Cranberry
can prevent E. Coli attaching to UT lining. However, it can
not remove the bacteria once it has already attached.
Main strength of cranberry against UTIs is its
antioxidant content.
In particular, the North
American cranberry Vacinnium Macrocarpon has been found to contain unique,
tannin-like A-linked PACs that prevent E. Coli from adhering to the cells lining
much of the urinary tract (including ureters, bladder, and parts of the urethra)
- helping to support UT, gastro-intestinal,
and oral health. Many fruits and vegetables contain PACs, however only Cranberry
A-type PACs have been shown to provide both anti-stick and antioxidant properties.
Studies report that other members of the Vaccinium genus also have similar
properties, including bilberry and blueberry. Cranberry
containsVitamin C
Problems with cranberry juice
Cranberry
creates an acidic urine conducive to E. Coli growth.
Not advisable to drink duringa UTI, which may involve E. Coli;
Cocktail
versions of cranberry juice contain added sugar. As food for bacterial growth;
Too much
cranberry can increase the likelihood of calcium-oxalate kidney stones.
This type of stone represents 75% of kidney stones in the U.S.
Cranberry
increases hippuric acid in the urine. Hippuric
acid can act as an irritant for an already inflamed bladder, and provides a ready
source of nutrition for pathogens that most commonly infect the upper and lower
urinary tract, bladder, and kidneys. Cranberry, because it feeds acid tolerant bacteria,
can be responsible for strengthening bacterial colony sizes and forcing E. Coli
in particular into 'burst rate' lifestyles, where they can utilize the hippuric
acid as an ideal growth medium. Bodel, Phyllis T. et al, 1959
Guidelines for consuming cranberry juice / extracts
Use only unsweetened 100% Cranberry Juice
(not cocktails)
There are synergistic benefits when
consuming the whole berry (lost using extracts). These include antioxidant,
anti-inflammatory, and anti-cancer benefits of cranberry;
Drink in moderation to deter calcium-oxalate
kidney stone formation and intake of excess sugar
Capsules of unsweetened cranberry juice powder
(standardized to contain 11-12% quinic acid; responsible for the tart taste
of cranberries) are many times more potent than
cranberry juice
The amount of PACs needed
for benefit is ~35 mg per day
Supplement should NOT contain binders.
Many cranberry supplements use cellulose or guar gum as binders to hold tablet
together, but the problem is that they also bind to the PACs in cranberries -the
active ingredient
Avoid postponing urination.
Urinate frequently and empty bladder completely.
Measures before and after sexual intercourse.
For women who experience bladder infections related to intercourse,the
recommendation is to take ½ tsp. d-mannose 1 hour prior to and just after
intercourse. Also urinate within 15 minutes after intercourse.Use a water-soluble
lubricant (E.g. K-Y Lubricating Jelly) during intercourse. Also, use female-superior
or lateral positions in sexual intercourse to protect the female urethra from injury.
Avoid FRAGRANCED bubble baths, douches, feminine
hygiene sprays or deodorants, tampons, toilet paper or soaps.
Chemicals can be irritating.
Chronic UTI sufferers should use sanitary pads
(preferably cotton-based) instead of
tampons
Clean anal area thoroughly after bowel movements
/ Wipe from the front to the rear. Rather
than rear to front to avoid spreading fecal bacteria to the genital area.
Use underwear or pantyhose with a cotton crotch
/ Avoid prolonged wearing of wet swimwear
Reduce stress.
Known to be immunosuppressive; acupuncture has shown good results against UTIs,
so therefore the Meridian Tapping Technique (MTT) would also be of benefit;
ANTHONY J. SCHAEFFER,* SUSAN K. AMUNDSEN, AND LAWRENCE
N. SCHMIDT (Jun 1979) Adherence of Escherichia coli to Human Urinary Tract Epithelial
Cells, INFECTION AND IMMUNITY: pgs 753-759
Pdf
article
Bodel, Phyllis T. et al (1959) Cranberry juice
and the antibacterial action of hippuric acid. The Journal of Laboratory and
Clinical Medicine , Volume 54 , Issue 6 , 881 - 888
Link
L. DOMENICI, M. MONTI, C. BRACCHI, M. GIORGINI, V. COLAGIOVANNI,
L. MUZII, P. BENEDETTI PANICI (2016) D-mannose: a promising support for acute urinary
tract infections in women. A pilot study. European Review for Medical and Pharmacological
Sciences. 20: 2920-2925
Pdf article
Ofek, I., E. H. Beachey, and N. Sharon. (1978) Surface
sugars of animal cells as determinants of recognition in bacterial adherence. Trends
Biochem. Sci. 3:159-160.
Abstract
Ofek, I., D. Mirelman, and N. Sharon. (1977) Adherence
of Escherichia coli to human mucosal cells mediated by mannose receptors. Nature
(London) 265:623-625.
Kranjcec B, Papes D, Altarac S.(Feb 2014) D-mannose
powder for prophylaxis of recurrent urinary tract infections in women: a randomized
clinical trial. World J Urol. 32(1):79-84.
PubMed
Wellens A, Garofalo C, Nguyen H, Van Gerven N, Slättegård
R, Hernalsteens JP, Wyns L, Oscarson S, De Greve H, Hultgren S, Bouckaert J. (Apr
30, 2008) Intervening with urinary tract infections using anti-adhesives based on
the crystal structure of the FimH-oligomannose-3 complex. PLoS One. 3(6): e2040.
Shields-Cutler RR, Crowley JR, Hung CS, Stapleton AE,
Aldrich CC, Marschall J, Henderson JP (2015, Jun 26) Human urinary composition
controls siderocalin'santibacterial activity. The Journal of Biological
Chemistry.
DISCLAIMER: The content on this website is intended for
informational, and educational purposes only and not as a substitute
for the medical advice, treatment or diagnosis of a licensed health
professional. The author of this website is a researcher, not a
health professional, and shall in no event be held liable to any
party for any direct, indirect, special, incidental, punitive or
other damages arising from any use of the content of this website.
Any references to health benefits of specifically named products
on this site are this website author's sole opinion and are not
approved or supported by their manufacturers or distributors.