Health Happening
The "No-Brainers" for Physical and Mental Health:
An imbalance of estrogen over PROGESTERONE in women (or TESTOSTERONE in men) is having an overall estrogenic effect. The most well-known repercussion of this is to cause overproliferation of cells resulting in reproductive organ cancers (e.g. breast, endometrial, ovarian and prostate), and issues, such as polycystic ovarian syndrome, uterine fibroids, fibrocystic changes in the breast and benign prostate hyperplasia.
The term "Estrogen Dominance" was coined by Dr. John R. Lee. An author, expert and pioneer in the study and use of PROGESTERONE and androgen supplementation to restore hormonal balance.
Estrogen Dominance is causing a myriad of health problems / symptoms in both women and men |
|
| ▪ Adrenal exhaustion | ▪ High blood pressure |
| ▪ Agitation / Anxiety / Panic disorders /Anger (unexplained) | ▪ Hypermenorrhea (heavy bleeding) |
| ▪ Aging accelerated | ▪ Hypoglycemia |
| ▪ Allergy symptoms (Asthma, hives, rashes, sinus congestion) | ▪ Increased blood clotting (risk of strokes) |
| ▪ Amenorrhea (skipped periods) | ▪ Infertility |
| ▪ Autoimmune disorders (increased risk) e.g. lupus erythematosis, thyroiditis, Grave's disease, possibly Sjogren's disease | ▪ Irregular /heavy bleeding |
| ▪ Bloating (water retention) | ▪ Irritability |
| ▪ Blood clotting excess (stroke) | ▪ Insomnia / Restless sleep |
| ▪ Blood clotting in lungs (i.e. pulmonary embolism) | ▪ Lethargy / Loss of esteem |
| ▪ Blood sugar irregularities | ▪ Magnesium deficiency |
| ▪ Breast cancer (hormone-sensitive type)* | ▪ Miscarriage (early) |
| ▪ Breast cancer in men (6000/yr in U.S.) | ▪ Mood swings |
| ▪ Breast tenderness / swelling | ▪ Obesity |
| ▪ BPH (Benign prostate hypertrophy) (Enlarged prostate) | ▪ Osteoporosis (reduced osteoblast bone-building function) |
| ▪ Copper retention/excess | ▪ Ovarian cancer (hormone-sensitive) |
| ▪ Cervical dysplasia (abnormal cells) | ▪ Oxygen reduction to cells |
| ▪ Chronic fatigue | ▪ Pain in joints / muscles |
| ▪ Cold hands and feet (as thyroid dysfunction) | ▪ Panic attacks |
| ▪ Cyclical headaches / Migraine | ▪ PMS |
| ▪ Decreased sex drive / libido | ▪ Polycystic ovaries (PCOS) |
| ▪ Depression with anxiety or agitation | ▪ Premenopausal bone loss |
| ▪ Dry eyes | ▪ Prostate cancer** |
| ▪ Dry or coarse skin | ▪ Pulmonary embolism |
| ▪ Early onset of menstruation | ▪ Restlessness |
| ▪ Early maturation in girls (breasts, pubic hair) | ▪ Sluggish metabolism / thyroid hormone activity interference |
| ▪ Endometriosis | ▪ Slurred or slow speech |
| ▪ Endometrial cancer risk increased |
▪ Sperm count reduced (up to 50%) |
| ▪ Erectile dysfunction / Impotency | ▪ Sweet craving |
| ▪ Fat gain, usually around abdomen, hips, thighs | ▪ Testicular tumors |
| ▪ Fatigue / low energy | ▪ Thyroid dysfunction mimicking hypothyroidism - makes thyroid receptor less sensitive to thyroid hormone. |
| ▪ Fibrocystic breast changes (FCC) | ▪ Uterine cancer (hormone-sensitive)* |
| ▪ Fibromyalgia | ▪ Uterine lining thickening |
| ▪ Fluid retention | ▪ Uterine cramping |
| ▪ Foggy thinking / decreased cognitive ability | • Uterine fibroids / fibroid tumors |
| ▪ Gallbladder disease | ▪ Vascular tone reduced |
| ▪ Gynecomastia(Enlarged breasts in men) | ▪ Vertigo |
| ▪ Hair loss / poor condition / Male pattern baldness | ▪ Weight gain (without explanation) |
| ▪ Headaches / migraine | ▪ Zinc deficiency / loss (negatively affects immune system, soft tissue repair) |
| ▪ Heart disease (heart attack, stroke, blood vessel spasms, HBP, lowers blood-oxygen carrying capacity) | ▪ Weight gain (without explanation) |
| ▪ Heart disease (heart attack, stroke, blood vessel spasms, HBP, lowers blood-oxygen carrying capacity) | ▪ Zinc deficiency / loss (negatively affects immune system, soft tissue repair) |
Note: A woman suffering from high estrogen levels during menopause will usually have an estrogen reading of 200+ pg/ml.
* Increased risk of breast and uterine cancer. Estrogen is thought to stimulate growth of those cells containing estrogen receptors by causing an increase in stimulatory growth factors (TGF-α) and a decrease in inhibitory growth factors (TGF-β). Dickson RB, Lippman ME, Estrogenic regulation of growth and polypeptide growth factor secretion in human breast carcinoma. Endocr Rev. 1987.
** Certain estrogen metabolites are involved in prostate cancer. 2010 study found that The relative amounts of the 15 estrogens and estrogen metabolites in the urine of prostate cancer cases were similar to that of non-cancer patients with the exception of the estrogen metabolite 4-OHE1. Interestingly, it was also found that the estrogen metabolites considered harmful in breast cancer (16-KE2 and 17-epiE3) are secreted in higher amounts among those without prostate cancer and in lower amounts in those with prostate cancer. It was suggested that these metabolites may have a protective role in prostate cancer, which should be further explored. Ourania Kosti et al, Urinary estrogen metabolites and prostate cancer risk: A pilot study. The Prostate April 2011 Volume 71,Issue 5,pages 507-516 Wiley Online
PROGESTERONE is essentially the "antidote" to estrogen. Men generate less estrogen than women, and so generally do not need as much of the PROGESTERONE "antidote".
| ESTRADIOL is: | PROGESTERONE is: |
| ▪ Inflammatory | ▪ Anti-inflammatory |
| ▪ Stimulates tissue growth | ▪ Sloughs off tissue |
| ▪ Neurostimulating | ▪ Calming |
| ▪ Immuno-supporting | ▪ Immuno-suppressive |
If estrogen levels stay unopposed by PROGESTERONE, any of several health disorders may develop. In particular, women experience many unpleasant symptoms when estrogen levels are high compared to PROGESTERONE, during menopause or the monthly menstrual cycle.
A healthy PROGESTERONE / ESTRADIOL (E2) ratio for a woman. Is~ 200-300 to 1. Breast or uterine cancer most often occurs in women with a PROGESTERONE / E2 ratio of less than 200 to 1.
A tragic illustration of the effects of estrogen without sufficient PROGESTERONE. The synthetic estrogen drug Premarin was prescribed for years to women without any accompanying PROGESTERONE, resulting in an epidemic of uterine cancer. This led to estrogen and PROGESTERONE (albeit synthetic versions with unpleasant side-effects) being prescribed in combination.
Comparison between Effects of Estrogen and PROGESTERONE |
|
| Estrogen Effects | PROGESTERONE Effects |
| ▪ Causes the womb lining to thicken | ▪ Causes the endometrium to shed |
| ▪ Increases body fat deposits | ▪ Burns body fat for energy |
| ▪ Triggers depression, anxiety, headaches | ▪ Acts as an anti-depressant |
| ▪ Stimulates breast tissue / Sore breasts | ▪ Protects breast tissue (e.g. against fibrocystic breast changes (FCC) ) |
| ▪ Decreased libido (also with a deficiency of estrogen) | ▪ Optimizes libido/Restores normal sexy feelings |
| ▪ Causes salt, sugar and fluid retention | ▪ Acts as a natural diuretic |
| ▪ Causes breast and prostate cancer; Increases risk of endometrial/uterine cancer ** | ▪ Helps prevent breast, endometrial, uterine cancer |
| ▪ Counteracts thyroid hormone action *** | ▪ Aids thyroid hormone action |
| ▪ Causes copper levels to increase/zinc to decrease | ▪ Helps to balance copper and zinc levels |
| ▪ Reduces oxygen supply to all cells - Estrogen shifts cells away from oxidative energy production (âž” cancer) | ▪ Corrects oxygen supply to cells |
| ▪ Increases risk of blood clotting | ▪ Normalizes risk of blood clots |
| ▪ Prolongs monthly bleed time | ▪ Normalizesperiod length |
| ▪ Acts as an abortive | ▪ Initiates/Sustains baby's survival throughout pregnancy |
| ▪ High corticosterone | ▪ Precursor of corticosterone production |
| ▪ Slows breaking down of bone by its rate-limiting effect on osteoclast function | ▪ Stimulates bone building by stimulating osteoblasts |
| ▪ Stimulates nervous system | ▪ Calms nervous system |
| ▪ Reduces blood vessel tone/ability to constrict or dilate | |
| ▪ Impairs blood sugar control | ▪ Normalizes blood sugar control |
** ESTRADIOL excess causes breast and prostate cancer. Newer studies show beyond debate that unopposed ESTRADIOL actually causes, not just increases the risk for breast cancer and prostate cancer.
*** Estrogen Dominance slows down metabolism causing hypothyroid symptoms, such as fat gain - The thyroid hormones T3 and T4 enter every cell in the body to stimulate protein synthesis and provide energy by utilizing calories; estrogen stores calories as fat. A surplus of estrogen triggers the liver to produce thyroid-binding globulin, which binds and neutralizes T3 and T4 in the blood. While the thyroid is producing sufficient amounts of hormone (tests are usually normal or just below normal) an insufficient amount of thyroid hormones is making it to the cells, such that an estrogen dominant person looks hypothyroid. E.g. thinning hair, low temperature, and increased fat on the hips and belly..
After 4-6 months of getting rid of xenoestrogens and phytoestrogens, and taking PROGESTERONE, the thyroid hormones are usually "back in business"
In aging men, estrogen levels increase as TESTOSTERONE and PROGESTERONE levels decrease. This occurs because TESTOSTERONE levels generally decline with age, and because the often increasing number of fat cells convert TESTOSTERONE to estrogen. Also weak testes produce less PROGESTERONE
Without ovulation, there is no ovarian corpus luteum to produce PROGESTERONE , and a PROGESTERONE deficiency ensues. Any estrogen present remains unopposed, yielding several unwantedside effects. Unfortunately, maladies such as water retention, weight gain, fatigue and depression are sometimes diagnosed as separate problems and treated individually, when actually, they are symptoms of a person with too much estrogen relative to other hormones. Today, research is showing that many women in their 30s and even younger are sometimes not ovulating during their menstrual cycle. Lee, 1993
Excessive intake of plant estrogens. Any additional estrogen by prescription or supplemented, will increase estrogen levels and must be properly balanced with natural PROGESTERONE - Typical sources of prescription estrogen are birth control pills and hormone replacement therapy.
Estrogen-mimicking phytoestrogens.
▪ High levels of soy generating anti-estrogeniceffect are equivalent to drinking three 12-ounce glasses of soy milk /dayfor a month - three 12oz glasses is 60g soy protein (equivalent to 45 mg of isoflavones);
▪ Excessive soybean consumption inhibits the thyroid and is widely associated with hypothyroidism - Asia has endemic hypothyroidism (China has 100,000,000 cretins).
It is now well-established that many phytoestrogens and hormone-disrupting chemicals exhibit an inverted-U "Dose to inhibitory response" curve |
|
Phytoestrogens and hormone-disrupting chemicals disrupt/inhibit hormones at low doses but not at high doses - What seems to happen is that the hormone system becomes overwhelmed and stops responding, so at high doses there is no observable effect. Traditional toxicological testing at high doses may miss important effects that only occur at lower doses. The Inverted "U Dose to inhibitory response curve. Initially, as a dose rises, the inhibitory response rises. However, at some point as the dose continues to rise the response stops rising, then begins to diminish and falls back toward zero. 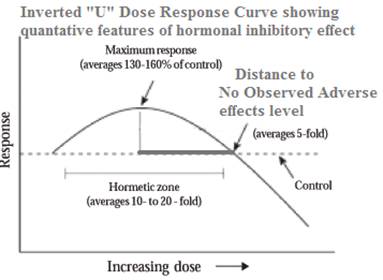 Examples of the Inverted U Dose-response curve:
|
TESTOSTERONE converts to ESTRADIOL via the aromatase enyme produced by fat cells;
Caffeine / Coffee / Alcohol / Nicotine. One study (Fertility and Sterility 2001;76:723-729) finds that drinking more than two cups of coffee daily may boost estrogen levels in women and could exacerbate conditions such as endometriosis and breast pain. The study included nearly 500 women aged 36 to 45 who were not pregnant, breast-feeding or takinghormones. All women answered questions about their diets, smoking habits, height and weight. Researchers measured the women's hormone levels during days 1 to 5 of their menstrual cycle.
Caffeine intake from all sources was linked with higher Estrogen levels. Regardless of age, body mass index (BMI), caloric intake, smoking, and alcohol and cholesterol intake.Women who consumed at least 500 mg of caffeine daily (E.g. 4 - 5 cups of coffee), had nearly 70% more estrogen during the early follicular phase than women consuming no more than 100 mg of caffeine daily (< 1 cup of coffee).
Smoking / Nicotine. Women aged 40 and older and those who smoked had higher levels of follicle stimulating hormone (FSH), which corresponds with fewer eggs remaining in a woman's ovaries. FSH tends to increase withage. Thus, the observation that smokers have higher FSH levels suggests that their ovaries are ``older'' than their chronological age.
Xenoestrogens (The Greek word xeno means foreign) are industrially made compounds with a molecular structure so similar to estrogen that they have estrogenic effects (i.e. stimulate estrogen receptors) in the body. xenoestrogens are having significant and serious effects on our health. Many endocrine-disrupting contaminants, even if less potent than the natural products, are present in living tissue at concentrations millions of times higher than the natural hormones. They are being blamed for increasing rates in hormone-sensitive breast, prostate and reproductive cancers, fibroids, cysts, reduced infertility, menopausal problems, PMS and early puberty in children.These endocrine disruptors create imbalances, especially in the reproductive, thyroid and adrenal systems. They can increase growth of the endometrium and disrupt the reproductive cycle. In the U.S., more than a quarter of all women are now having hysterectomies by the age of 60. Even men are not exempt from their effects, with many being diagnosed with BPH and complaining of declining sexual performance.
Xenoestrogens are strong and long-lasting. These chemicals bind permanently to receptor sites, accumulate in fat tissues, and disrupt nearly every biological process. Small daily doses build up, leading to an unbalanced endocrine system. Obesity and adrenal exhaustion (chronic fatigue/"stress") follow.
The environmental background of xenoestrogens provides a continuous estrogenic exposure. Unfortunately these modern day "Estrogen look-alikes"are nearly impossible to avoid since they are ubiquitously present in our lives, in meat and dairy, food preservatives, personal care products, household goods, herbicides, pesticides, fertilizers, plastics, and more.However, it is possible to reduce your exposure to xenoestrogens if you know where to find them, so brace yourself for a depressing revelation as these sources are revealed:
X-rated xenoestrogens - Endocrine Disruptors
PROGESTERONE is necessary to counterbalance estrogen and TESTOSTERONE
Women who do not ovulate during their cycle will not produce any PROGESTERONE that cycle. This is a common occurrence and worsens the already disturbed PROGESTERONE / estrogen balance;
PROGESTERONE production is reduced in menopause. Only the adrenal gland is producing it, because a woman is no longer ovulating.
| Symptoms of PROGESTERONE Deficiency | ||
|---|---|---|
| • Recurrent early miscarriage | • No period | • Not ovulating |
| • Endometriosis | • PCOS | • PMS |
| • Cramps during menses | • Blood Clotting | • Swollen Breasts |
| • Fibrocystic breasts | ||
Lack of available cholesterol for PROGESTERONE synthesis. The corpus luteum depends almost exclusively on peripheral low-density-lipoprotein-carried cholesterol (LDL-cholesterol)for making steroids. Gwynne JT.; Strauss JF, 1982
Although such decreases in PROGESTERONE levels were not significant, it is likely that dosage of vitamin E greater than 600 IU will result in greater PROGESTERONE suppression. This may explain why PMT-A (most common type of premenstrual tension) symptoms worsened with 600 IU of vitamin E whereas 150 IU showed an improvement of PMT-A symptoms. London RS et al, 1983

Inhibition of PROGESTERONE synthesis by the prostaglandin PGF2a. PGF2a is luteolytic (Degrades corpus luteum) in women. Dennefors BL et al, 1982
| Dr. Guy Abraham's thoughts on effects of Vitamin E on PGF2a |
|---|
| The luteotropic effect (stimulating formation of corpus luteum of small doses of vitamin E (150 IU or less) could be due to the inhibitory effect of vitamin E on the release of AA from storage pool, in this manner decreasing the availability of PGF2a precursors. The net effect of vitamin E on PROGESTERONE synthesis would depend on the response of LDL-cholesterol and arachidonate release from storage pools to various dosages of vitamin E. It is possible that blockage of arachidonate release is more sensitive to vitamin E than suppression of LDL-cholesterol, such that low dose of vitamin E would decrease precursor availability for PGF2a synthesis (a luteotropic effect) and high dose of vitamin E would suppress LDL cholesterol (a luteolytic effect). |
Stress reduces PROGESTERONE function - when under stress, the adrenals pump out CORTISOL, which blocks some PROGESTERONE receptors and thus prevents PROGESTERONE function.
Chronic stress uses up our available PROGESTERONE. Chronic stress will cause adrenal fatigue, prompting the body to go to "Plan B"and use available PROGESTERONE to make CORTISOL. However, in this scenario, there is not enough PROGESTERONE to make the needed TESTOSTERONE for a woman's sexual response, never mind to oppose rising levels of estrogen. No wonder a woman feels lethargic and disinterested in sex when stressed!
It is not uncommon for women to experience menstrual cycles without ovulating as many as 10 years before menopause. In those cycles enough estrogen is made to create menstruation, but not enough PROGESTERONE to balance it. Even after menopause, the estrogen ESTRONE, ccontinues to be produced in the fat cells, while PROGESTERONE production is greatly diminished, since the ovaries are no longer producing and the job is left to the adrenal glands.
A healthier liver takes up, degrades and excretes excess estrogen, xenoestrogens and sex hormone-binding globulin (SHBG) in bile or urine. A weak liver that fails to eliminate these surpluses in the body is often responsible for hormonal abnormalities.
Excessive alcohol consumption. Blocks the liver enzyme that breaks down estrogen. Overindulging raises estrogen levels in both men and women;
Diseases of the liver. Cirrhosis (lesions in the liver) or decreased enzyme activity can lead to increased estrogen levels;

Vitamin B6, magnesium, zinc and / or B2 deficiency. B6 is an important cofactor for enzymes necessary for the liver to conjugate estrogens from the blood. A B6 deficiency affects the liver's estrogen clearance, keeping blood estrogen levels high. MS and Biskind, GR, 1942; Biskind, M.S, 1943; Biskind; MS and Biskind, GR, 1945; Biskind et al, 1944
Magnesium also has a direct role in estrogen conjugation. By increasing the activity of an enzyme (glucuronyl transferase) involved in the liver's glucuronidation of estrogens. Abraham GE, 1984

Aging and Certain Drugs. Impair liver function;
Iodine deficiency causes estrogen imbalance. Iodine directly controls how much estrogen is produced by the body and in some cases the lack of iodine might cause a surge in the production of the estrogen;
Iodine supports natural cell death in the breasts and ovaries in a woman's monthly reproductive cycle - In preparation for pregnancy each month, there is a build up of cells in the breasts and uterus. When conception does not occur, the body rids itself of these then unneeded cells by a natural monthly "programmed cell death", called apoptosis.Not having appropriate monthly apoptosis can lead to fibrocystic breasts, polycystic ovarian syndrome or endometriosis.
Some studies supporting anti-Estrogenic effect of iodine
Typically seen in a diet heavy in artificial ingredients and refined sugar and flour
High fat, carbohydrate rich diet and resultant weight gain raises estrogen levels. An enzyme in fat cells converts adrenal hormones to Estrogens.
(1) Too little PROGESTERONE. Occurs when PROGESTERONE production ceases or is suppressed. This creates a situation of estrogen dominance, and is the most common reason for miscarriage. Factors influencing lower PROGESTERONE levels include:
(2) Too much estrogen. Much of today's increase in estrogen levels in women is due to:
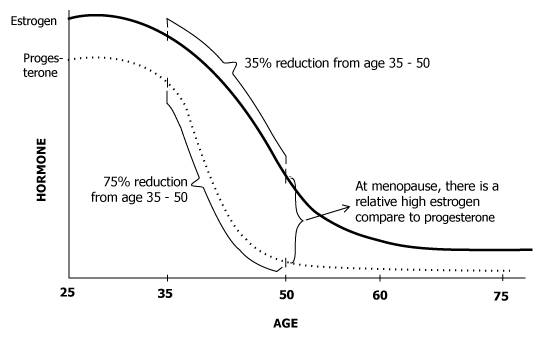
(3) In aging and menopause PROGESTERONE levels fall faster than estrogen. Estrogen levels in women whose ovaries are no longer functioning will remain at approximately 40% of their former concentration levels. This is because most women continue to produce estrogen by conversion of androgens (derived from the adrenal gland) into estrogen in the fat cells. PROGESTERONE concentration levels, however, drop to almost zero (1/120 of the former levels). Doing the math, this means that the ratio between estrogen and PROGESTERONE has increased by a factor of 50.
(1) Too little TESTOSTERONE
(2) Too much estrogen. Most commonly caused by factors such as:
(3) Too little PROGESTERONE
Understanding the changingestrogenand TESTOSTERONE levels in men
Do you have an estrogen deficiency? - Any woman still having monthly periods has plenty of estrogen. On the other hand, vaginal dryness , vaginal mucosal atrophy night sweats, hot flashes, and emotional rollercoaster rides are clear signs of estrogen deficiency. Lacking these signs, the most accurate and reliable test today is the saliva hormone assay.
Symptoms of LOW Estrogen Levels(particularly in menopausal women) |
|
▪ Severe depression/Anger |
▪ Difficulty concentrating |
▪ Hot Flashes |
▪ Joint / muscle Pain |
▪ Night Sweats |
▪ Vaginal Dryness and Vaginal/bladder infections |
▪ Memory Lapses |
▪ Dry skin / Skin aging |
▪ Heart palpitations |
▪ Dizziness |
▪ Fatigue |
▪ Loss of breast tone |
The most common long-term symptom / side effect of LOW estrogen levels is osteoporosis - thought to be present in 20% of post menopausal women. Estrogen deficiency makes osteoclasts more sensitive to the hormone that causes bone resorption:
In postmenopause, the positive effects of estrogen on growth factors, CALCITONIN, vitamin D metabolism, and calcium absorption are diminished
Circulating levels of estrogen
Symptoms of High Estrogen Levels in Women |
|
| Physical | Psychological |
| ▪ Headaches | ▪ Mood Swings |
| ▪ Weight Gain | ▪ Anxiety |
| ▪ Breast tenderness | ▪Depression |
| ▪ Irregular periods | ▪ Loss of Libido |
| ▪ Water retention / Bloating | ▪ Insomnia |
| ▪ Hypoglycemia | |
| ▪ Gallbladder problems | |
(typically together with low TESTOSTERONE levels in men and low PROGESTERONE levels in women. A woman suffering from high estrogen levels during menopause will usually have an estrogen reading of 200+ pg/ml)
Stimulates cell growth
Certain estrogen metabolites involved in prostate cancer. 2010 study found that the relative amounts of the 15 estrogens and estrogen metabolites in the urine of prostate cancer cases were similar to that of non-cancer patients with the exception of the estrogen metabolite 4-OHE1. Interestingly, it was also found that the estrogen metabolites considered harmful in breast cancer (16-KE2 and 17-epiE3) are secreted in higher amounts among those without prostate cancer and in lower amounts in those with prostate cancer. It was suggested that these metabolites may have a protective role in prostate cancer, which should be further explored. Ourania Kosti et al, 2011
Ourania Kosti et al, Urinary estrogen metabolites and prostate cancer risk: A pilot study. The Prostate April 2011 Volume 71,Issue 5,pages 507-516 Wiley Online
Increase risk of cardiovascular disease
Promotes blood clots in the lungs (i.e. pulmonary embolism)
Implicated as a cause of benign prostatic hypertrophy (BPH)
Depletes body's zinc - negatively affecting:
The treatment objective is NOT to RESTORE your hormone levels to those of a person in their 20s or 30s (E.g. A menopausal woman no longer needs the higher hormone levels required for reproduction). The goal is to correct a hormonal imbalance in the main sex hormones that may be wreaking havoc with many of the body's systems and causing serious health problems. Specifically, the treatment corrects an imbalance of:
Benefits of correcting this imbalance can:
Who may need treatment for estrogen dominance?
Treatment for estrogen dominance involves 3 steps.
The first approach to an estrogen dominance over PROGESTERONE (in women) or TESTOSTERONE (in men) is to reduce estrogen levels in the body:
Help adrenal glands increase their PROGESTERONE production. The innermost layer of the adrenal glands produces small amounts of the sex hormones (Androgens, estrogensand PROGESTERONE)
Try and reduce stress. Stress uses up PROGESTERONE. When under stress, most of the PROGESTERONE produced by the body is converted into the corticosteroid hormones to deal with emotional stress or fight or flight situations. This creates an estrogen dominance situation leading to insomnia and anxiety, which further taxes the adrenals, and a vicious cycle continues as PROGESTERONE is used to make stress hormones. Weakened adrenal glands will never allow the hormones to find proper equilibrium
Balance Adrenal "Stress Management"Glands
But only AFTER using above tactics to reduce estrogen and naturally increase PROGESTERONE
PROGESTERONE supplementation may be beneficial when you are living today's 'Typical' lifestyle. It helps to counter-balance an excess estrogen presence. However, decreasing the body's estrogen levels should always be the first approach.
How does PROGESTERONE counter estrogen?
PROGESTERONE desensitizes the estrogen receptors;
How to supplement PROGESTERONE
Estrogen reduces thyroid function by increasing thyroid binding globulin (TBG), which binds thyroid hormone making it inactive. This provides an explanation for why hypothyroid symptoms are similar to estrogen dominance symptoms
Iodine - The Universal Medicine
http://www.johnleemd.com/store/resource_hormonetest.html
The Estrogen Alternative: A guide to Natural Hormone Balance
Interview with Dr. Lee http://www.keepsmilin.com/transcriptdrlee.htm
Abraham, G.E.; Schwartz, U.D.; Libran, M.M.: Effect of vitamin B-6 on plasma and red blood cell magnesium levels in premenopausal women. Ann. clin. Lab. Sci. 11: 333 (1981).
Abraham GE. Nutrition and the premenstrual tension syndromes, J Appl Nutr, 1984; 19:57-63
Biskind, M.S.: Nutritional deficiency in the etiology of menorrhagia, cystic mastitis and premenstrual tension. Treatment with vitamin B complex. J. clin. Endocr. Metab. 3: 227-234 (1943).
Biskind, M.S.; Biskind, G.R.: Effect of vitamin B complex deficiency on inactivation of ESTRONE in the liver. Endocrinology 31: 109-114 (1942).
Biskind, M.S.; Biskind, G.R.: Inactivation of TESTOSTERONE propionate in the liver during vitamin B complex deficiency. Alteration of the estrogen-androgen equilibrium. Endocrinology 32: 97-102 (1945).
Biskind, MS.; Biskind, GR.: Biskind, L.H.: Nutritional deficiency in the etiology of menorrhagia, metrorrhagia, cystic mastitis, and premenstrual tension. Surgery Gynec. Obstet. 78: 49-57 (1944)
Cowan LD et al. Breast cancer incidence in women with a history of PROGESTERONE deficiency. Am. J. Epidem. 114: 209 (1981).
Dennefors BL et al. PROGESTERONE and adenosine 3', 5'- monophosphate formation by isolated human corpora lutea of different ages. Influence of human chronic gonadotropin and prostaglandins. J. clin. Endocr. Metab. 55: 102 (1982)
Dickson RB, Lippman ME, Estrogenic regulation of growth and polypeptide growth factor secretion in human breast carcinoma.Endocr Rev.1987
Gwynne, J.T.; Strauss, J.F., III: The role of lipoproteins in steroidogenesis and cholesterol metabolism in steroidogenic glands. Endocr. Rev. 3: 299 (1982).
Lee, John R., M.D. (1993) Natural PROGESTERONE : The Multiple Role of a Remarkable Hormone, BLL Publishing, California, USA p.29.1
London, R.S.; Sundaram, G.S.; Murphy, L.; et al.: The effect of alpha-tocopherol on premenstrual symptomatology. A double-blind study. J. Am. Coil. Nutr. 2: 115 (1983)
London RS et al.: The effect of alpha-tocopherol on premenstrual symptomatology. A double-blind study. H. Endocrin correlates. J. Am. Coll. Nutr. 3: 351 (1984)
Murray RK et al. Harper's Biochemistry. 23rd ed. Norwalk CN:Appleton & Lange; 1993
Ourania Kosti et al, Urinary estrogen metabolites and prostate cancer risk: A pilot study. The Prostate April 2011 Volume 71,Issue 5,pages 507-516 Wiley Online
Raymond F. Peat (Jul 1995) Estrogen: Simply Dangerous, Ray Peat's newsletter
Stadel BV, Dietary iodina and risk of breast, endometrial, and ovarian cancer, Lancet,1976;
Wynder EL et al. Nutrition and the etiology and prevention of breast cancer; in Strax, Control of breast cancer through mass screening, pp. 89-100 (Littleton, Colorado 1979)








