Health Happening
The "No-Brainers" for Physical and Mental Health:

 (2) ELIMINATE
(2) ELIMINATE


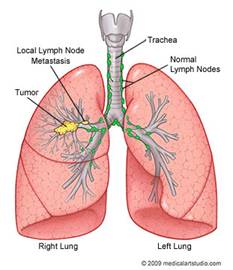
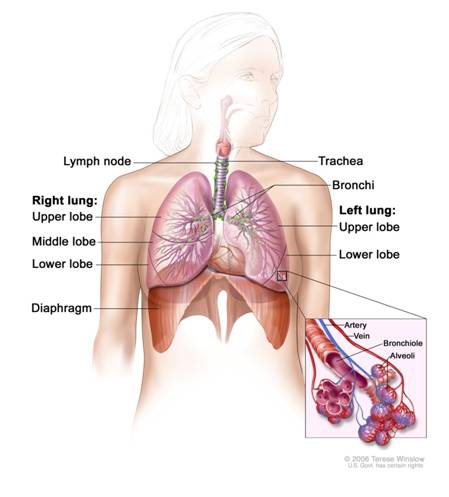
Cancer that forms in tissues of the lung - usually in the cells lining air passages
Age-Related Causes of Death in Women |
|||||
|
Age |
Heart Disease |
Cancer |
Lung |
Breast |
Colorectal (Colon) |
|
15-34 |
#1 | ||||
|
35-54 |
#2 |
#1 |
#1 | ||
|
55-74 |
#2 |
#1 |
#1 |
#2 | |
|
>74 |
#1 |
#1 |
#3 |
#2 |
Race-Related Causes of Cancer Death in Women(rates per 100,000 women of all races) |
|||
|
Race \ Cancer Type |
Lung (39.0) |
Breast (22.5) |
Colorectal (13.8) |
|
White, black, American Indian/Alaska Native women. |
#1 |
#2 |
#3 |
|
Hispanic |
#2 |
#1 |
#3 |
Geographical Variations in Lung Cancer IN U.S.(rates per 100,000) |
||||
|
|
Women |
Men |
||
|
Incidence |
Death rate |
Incidence |
Death rate |
|
|
U.S. |
54.5 |
39.0 |
79.5 |
64.0 |
|
Northeast |
57.8 |
38.2 |
78.2 |
59.4 |
|
West |
45.5 |
33.8 |
60.4 |
49.2 |
|
Midwest |
57.3 |
42.4 |
83.2 |
69.1 |
|
South |
56.3 |
40.4 |
89.3 |
72.1 |
(U.S. Cancer Statistics Working Group, 2012)
The two types are distinguished by the appearance of the cancer cells under a microscope.

NSCLC grows more slowly than SCLC and accounts for almost 90% of all lung cancers
3 main sub-types of NSCLC:
NSCLC is sometimes treated with surgery. When non-small-cell lung cancer is found before it spreads beyond one lung, surgery can sometimes offer a cure. The surgeon may remove the part of the lung that contains the tumor, or if necessary, an entire lung. Some patients are given radiation therapy and/or chemotherapy after surgery to kill any remaining cancer;
SCLC is more aggressive than NSCLC and is strongly tied to cigarette smoking. Rarely seen in non-smoker; can quickly spread to other parts of the body early on.
SCLC usually responds better to chemotherapy and radiation. Surgery is not usually an option because it has typically already spread at the time of diagnosis. (Chapman et al, 2009)
At present, there is no effective medical therapy in metastatic Non Small Cell lung cancer (NSCLC) patients who progress under a first-line chemotherapy containing cisplatin. The following alternative treatments are provided, some with anecdotal success, others with supportive studies.
It is easy to KILL the cancer cells in a lung cancer patient - however, it is NOT SO EASY TO DO IT SAFELY without causing dangerous congestion in the lungs due to:
1. Dead cancer cell debris
2. Inflammation and swelling as a consequence of treatment. A dying cancer cell induces an immune system attack that causes inflammation and swelling.
Immune system (IS) building treatments do not cause inflammation, but are slow (up to 12 months). These type of treatments allow the IS to kill the cancer cells safely and are generally used in conjunction with proteolytic enzymes, which strip the protective protein coating from around the cancer cells so the IS can more easilykill the cancer cells. However, proteases thin the blood, so only moderate doses can be taken (e.g. 15 capsules a day of Vitalzym). The problem is that lung cancer patients typically do not have enough time for this method to work.
Any cancer treatment that kills cancer cells directly creates inflammation and is a balancing act between killing too many cancer cells (creating too much debris) and not killing enough (such that the cancer cells cause too much congestion). This can be very tricky and ideally needs clinical supervision. Fortunately, there are some fast-acting alternative treatment methods that do NOT cause inflammation and for lung cancer these are the best choices and they avoid the problem of creating congestion.
(Does not cause Inflammation or Congestion in lungs)
![]() (1) Cancer Treatment CORE
- Cancer NOT Allowed!
(1) Cancer Treatment CORE
- Cancer NOT Allowed!
Therapies of special mention included in:
![]() CANCER
TREATMENT CORE
CANCER
TREATMENT CORE
Baking soda / Maple Syrup Protocol. Baking soda alkalizes cells. Researchers have found that this protocol inhibits malignant growth by increasing tumor pH, and also reduces formation of spontaneous metasases. The sudden pH increase kills the cancer cells. as the shock of alkalinity allows more oxygen into the cancer cells than they can tolerate. (OR If, like this author,you hold with the microbial theory of cancer, it causes cancer microbe inside cells to die or go into its hibernating form, such that cells revert to normal metabolism. Baking Soda / Maple Syrup against Cancer
Magnesium against Cancer Without sufficient magnesium, the body accumulates toxins and acid residues and degenerates rapidly. For any degenerative disease, especially cancer, transdermal or nebulized magnesium chloride is a "No-brainer" to quickly build up the body's magnesium levels.
Alkalizing therapy to attend to Acid / Alkaline Balance - Nebulizing Sodium Bicarbonate is the best way to directly target the lungs
If a patient's lung cancer displays estrogen receptors, then reducing estrogen levels in the body, in addition to standard treatments, is potentially beneficial (since estrogen stimulates cancer growth). According to American Association for Cancer Research study published in 2002, human non small cell lung cancer show estrogen receptors and respond to estrogen. Estrogen dominance is a prevailing problem in today's world. (A receptor is a structure on the surface of a cell that selectively receives and binds substances). Laura P Stabile et al, 2002
"Our studies continue to show that lung cancer cells grow in response to estrogen and that stopping or slowing the spread of the disease may be dependent on blocking the action of estrogen, in fact, in previous studies, we have observed that lung tumor cells contain estrogen receptors at levels comparable to breast cancer cells."
- Jill Siegfried, Ph.D., professor, department of pharmacology and co-leader,Lung and Thoracic Malignancies Program, University of Pittsburgh Cancer Institute.
DIM supplementation proven to be beneficial in reducing estrogenic activity in the body. DIM demonstrated anti-cancer mechanisms in lung cancer in mice and human studies. Morse MA et al, 1990; Ichite N et al, 2009
I3C / DIM - Estrogen Blocker with Anti-cancer benefits
MELATONIN has multiple anti-estrogen actions and decreases estradiol levels in the body in lung cancer.
Vitamin K2 - For Klotting and Kalcium reduces estrogenic activity in body. Vitamin K2 (menaquinone) decreases the ratio of estradiol to less estrogenic estrone. Known for its blood coagulation effects, K2 also reduces estrogenic activity. Otsuka M et al, 2005
Estrogen levels lowered by maintaining healthy body weight. Body fat is a source of estrogen, therefore it is important to establish and maintain a healthy body weight. Siiteri PK, 1987
Progesterone therapy to deal with estrogen dominance in lung cancer
Chapman, S; Robinson G, Sradling J, West S (2009). "31". Oxford Handbook of Respiratory Medicine (2nd ed.). Oxford University Press. ISBN9-780199-545162
Collins LG, Haines C, Perkel R, Enck RE (January 2007). "Lung cancer: diagnosis and management". American Family Physician (American Academy of Family Physicians) 75(1): 56-63.
Study in The Lancet Oncology (2001)
U.S. Cancer Statistics Working Group (2012). United States Cancer Statistics: 1999-2008 Incidence and Mortality Web-based Report. Atlanta (GA): Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; http://www.cdc.gov/uscs.
WHO (February 2006). "Cancer". World Health Organization. Retrieved 2007-06-25;
Ichite N, Chougule MB, Jackson T, Fulzele SV, Safe S, et al. Enhancement of docetaxel anticancer activity by a novel diindolylmethane compound in human non-small cell lung cancer. Clin Cancer Res. 2009;15:543-552. PubMed
Laura P. Stabile, Autumn L. Gaither Davis, Christopher T. Gubish, Toni M. Hopkins, James D. Luketich, Neil Christie, Sydney Finkelstein and Jill M. Siegfried. Human Non-Small Cell Lung Tumors and Cells Derived from Normal Lung Express Both Estrogen Receptor α and β and Show Biological Responses to Estrogen. Cancer Res April 1 2002 (62) (7) 2141-2150; Link
Levin RD, Daehler MA et al. Circadian function in patients with advanced non-small-cell lung cancer. Br J Cancer. 2005 Nov 28;93(11):1202-8.
Lissoni P, Barni S, Ardizzoia A, et al. Randomized study with the pineal hormone melatonin versus supportive care alone in advanced nonsmall cell lung cancer resistant to a first- line chemotherapy containing cisplatin. Oncology 1992;49(5):336-339. View Abstract
Lissoni P, Giani L et al. Biotherapy with the pineal immunomodulating hormone melatonin versus melatonin plus aloe vera in untreatable advanced solid neoplasms. Nat Immun. 1998;16(1):27-33.
Lissoni P, Barni S et al. Decreased toxicity and increased efficacy of cancer chemotherapy using the pineal hormone melatonin in metastatic solid tumour patients with poor clinical status. Eur J Cancer. 1999 Nov;35(12):1688-92.
Lissoni P, Chilelli M et al. Five years survival in metastatic non-small cell lung cancer patients treated with chemotherapy alone or chemotherapy and melatonin: A randomized trial. J Pineal Res. 2003a Aug;35(1):12-5.
Lissoni P, Malugani F et al. Reduction of cisplatin-induced anemia by the pineal indole 5-methoxytryptamine in metastatic lung cancer patients. Neuro Endocrinol Lett. 2003b Feb;24(1-2):83-5.
Lynch E. Melatonin and cancer treatment. European Biology and Bioelectromagnetics. 2005 Jun 18;1(2):183-200.
Mazzoccoli G, Giuliani A et al. Decreased serum levels of insulin-like growth factor (IGF)-I in patients with lung cancer: Temporal relationship with growth hormone (GH) levels. Anticancer Res. 1999 Mar;19(2B):1397-9.
Moody TW, Chiles J et al. SR48692 is a neurotensin receptor antagonist which inhibits the growth of small cell lung cancer cells. Peptides. 2001 Jan;22(1):109-15.
Moody TW. Peptide hormones and lung cancer. Panminerva Med. 2006 Mar;48(1):19-26.
Morse MA, LaGreca SD, Amin SG, Chung FL. Effects of indole-3-carbinol on lung tumorigenesis and DNA methylation induced by 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) and on the metabolism and disposition of NNK in A/J mice. Cancer Res. 1990;50:2613-7. PubMed
Otsuka M, Kato N et al. Vitamin K2 binds 17beta-hydroxysteroid dehydrogenase 4 and modulates estrogen metabolism. Life Sci. 2005 Apr 8;76(21):2473-82.
Rato AG, Pedrero JG et al. Melatonin blocks the activation of estrogen receptor for DNA binding. FASEB J. 1999 May;13(8):857-68.
Sanchez-Barcelo EJ, Cos S et al. Melatonin-estrogen interactions in breast cancer. J Pineal Res. 2005 May;38(4):217-22.
Siiteri PK. Adipose tissue as a source of hormones. Am J Clin Nutr. 1987 Jan;45(1 Suppl):277-82.








