ESTRONE(E1), ESTRADIOL (E2) and ESTRIOL(E3) fluctuate with life stage. Suggesting specific roles for them in biological and disease processes.
- Fluctuations of ovarian hormones in perimenopause consist of intermittent high and low ESTRADIOL (E2) levels, followed eventually by chronically lower levels, and the predominance of ESTRONE (E1). These changes can be correlated with behavioral & other disturbances and pubertal and menstrual cycle-based fluctuations.
Changing levels of these estrogens could be instrumental in tissue development, function, and some lifestage-specific diseases in women
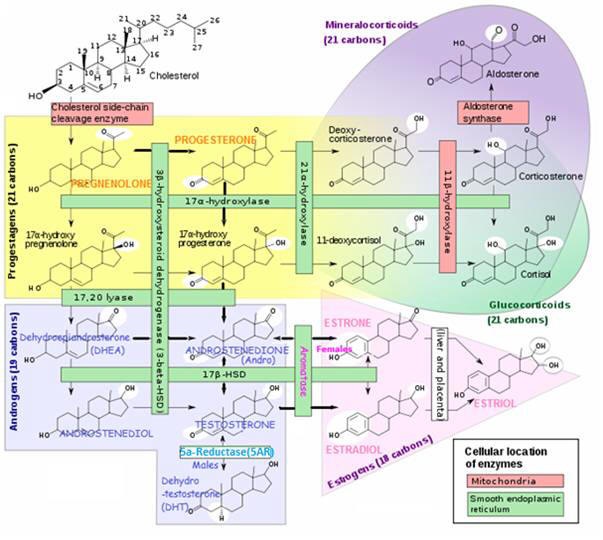
ESTRADIOL, ESTRONE and ESTRIOL are produced by aromatase enzymes in non-reproductive tissues (E.g. brain, fat cells). With possible effects on non-reproductive functions.
• E.g. ESTRIOL (E3) has protective effects against the development of arthritis in certain experimental models -as demonstrated for ESTRADIOL (E2)
• These estrogens could make a difference. In the brain, bone, cardiovascular system and many other tissues during different life stages.
- ESTRADIOL (E2, 17ß-ESTRADIOL)
• The predominant form in NON-pregnant females from menarche to menopause
• The most powerful and most carcinogenic.
- ESTRONE (E1)
• Produced and more predominant during menopause
• 70% less biologically active than ESTRADIOL
• ESTRONE (E1) is a significantestrogenic hormone contributor in both reproductive (0.5-1 nM) and postmenopausal (150-200 pM) women and in men;
- ESTRIOL (E3)
• Comprises nearly 80% of the total free estrogenin the female body
• Produced during PREGNANCY in much greater quantities than ESTRONE and ESTRADIOL - 10-100 nM in pregnant women and <7 nM non-pregnant women Decreased ESTRIOL (E3) levels in pregnancy have been associated with complications of eclampsia and the incidence of Down's syndrome in offspring.
The physiological effects of estrogens are mediated by the intracellular estrogen receptors (ERs). In response to estrogens, xenoestrogens and signals emanating from growth factor signalling pathways, they regulate:
(i) Genomic pathway initiation of gene expression (transcription) of target genes (for protein synthesis)
(ii) Non-genomic pathway functions
Specific effects of estrogens depend on:
• ER subtype in tissue ( ER-αand ER-β). E.g. ER-αpredominates inthe uterus and mammary gland, whereas ER-β has significant roles in the central nervous, cardiovascular, and immune systems; urogenital tract, bone, kidney, and lungs;
• Number of receptors - varies by location and whether pre- or post-menopause
ESTRONE(E1) and ESTRIOL(E3) are STRONG estrogens in the NON-genomic signaling pathways and functional pathways of pituitary
Watson CS, Jeng YJ, Kochukov MY. Nongenomic actions of ESTRADIOL compared with estrone and estriol in pituitary tumor cell signaling and proliferation. FASEB J. 2008 Sep;22(9):3328-36. doi: 10.1096/fj.08-107672. Epub 2008 Jun 9. PubMed
ESTRONE(E1) and ESTRIOL(E3) are WEAK estrogens in the GENOMIC pathway (affecting nuclear transcription activity)
ESTRADIOL (E2) is STRONG in the GENOMIC and NON-genomic pathways - although ESTRADIOL (E2) (in the high pM to nM range) is the physiological estrogen most often associated with GENOMIC pathways in female reproduction and the development of cancers in reproductive tissues.
- ESTRADIOL(E2) is stronger than ESTRONE(E1) and ESTRIOL(E3) in cell proliferation - E2 effects were evident at fM (Femtomolar - 1.0 fM is 1 million times smaller than a nM ) levels, whereas E1 and E3 were effective at 1 pM and 0.1 nM and above, respectively.